Management of incontinence
Lifestyle modifications and interventions
Lifestyle factors associated with urinary incontinence and stress incontinence in particular, include obesity (an independent risk factor), smoking, heavy lifting, high-impact activity, and constipation.
Abdominal adiposity increases intra-abdominal pressure, secondarily increasing intravesicular pressure and urethral mobility, resulting in incontinence. Thus, such patients should be referred for a weight loss programme; studies show that even a 5-10% weight loss resulted in marked improvement of incontinence (14). Obese women who lose significant amounts of weight before surgery may find that weight loss reduces the severity of their symptoms and obviate the need for surgery. At the very least, patients should be encouraged to lose weight preoperatively. A behavioural weight loss intervention should be considered the first-line treatment for overweight and obese women reporting stress incontinence (15). Weight loss and lifestyle interventions may also reduce the prevalence of incontinence in type 2 diabetics who are at increased risk for UI. Women should be encouraged to rationalize their fluid and caffeine intake and to give up smoking; the latter is another independent risk factor for SUI. Chronic constipation may cause pelvic floor muscle damage either directly or indirectly via pudendal nerve damage. These patients are also at a higher risk of recurrence following surgery. Hence dietary modifications such as a higher-fibre diet, laxatives, and stool softeners should be considered.Non-pharmacological-role of pelvic floor physiotherapy/biofeedback
The mechanisms of action of pelvic floor muscle training (PFMT) are by strength training and counterbalancing. PFMT improves urethral resistance and pelvic visceral support, including urethral support, primarily by increasing the strength of the voluntary pelvic floor muscles.
Additionally, voluntary contraction of the PFM precedes the increase in intra-abdominal pressure preventing urinary leakage (16). A focused regimen of PFMT is thought to act by changing the morphology and position of the muscles to enable subconscious contraction similar to continent women (17.) At least 4 months of PFMT are recommended to see tangible results; the improvement in the first 6-8 weeks is mainly caused by neural adaptation which is then followed by muscle hypertrophy, a process that continues over several months (18). PFMT is best administered by a trained physiotherapist and is an excellent first-line treatment for UI. If no improvement is noted after 6 months, the patient should consider alternative management strategies. Biofeedback may be considered in the subset of women who are unable to contract their pelvic floor muscles and therefore are unable to reliably perform PFMT. Biofeedback apparatus such as vaginal cones, manometry, and electromyography are commonly used to assist with PFMT.Timed or scheduled voiding is a programme developed to increase intervals between voids to attempt to suppress urgency and decrease incontinence episodes. The theory behind pelvic floor muscle retraining for urgency UI is based on the observation that a detrusor contraction can be inhibited by pelvic floor muscle contraction. Increasing the strength of the pelvic floor and ability of an individual to hold a contraction can result in extra time (perhaps just a few more seconds) to reach the toilet and avoid leakage (19).
Pharmacotherapy
Antimuscarinic medications have been used as second-line treatment of OAB symptoms, none is clearly more effective than the others and all have the tendency to cause distressing side effects (20). The clinician should therefore individualize treatment based on product and patient characteristics.
There are five known subtypes of muscarinic receptors within the bladder of which M2 and M3 subtypes predominate. Stimulation of the M2 receptor inhibits relaxation of the detrusor muscle, while activation of M3 receptors results in detrusor contractions (Figure 57.2).
Antimuscarinic agents (anticholinergics) have been developed to act on these two receptors. Antimuscarinic drugs including trospium, solifenacin, fesoterodine, tolterodine, and oxybutynin reduce the perception of urinary urgency and improve continence. Side effects were commonest with non- selective antimuscarinics such as oxybutynin and least common with solifenacin. Side effects commonly include dry mouth, constipation, and blurred vision. These drugs are contraindicated in patients with narrow-angle glaucoma and also carry the risk of urinary retention and should be used with caution in individuals with chronic open-angle glaucoma. Similarly, these drugs may precipitate urinary retention in patients with bladder neck obstruction. The bladder contains both alpha-adrenergic and beta- adrenergic receptors and stimulation of these receptors can exert some influence on the bladder and urethra. In the past couple of years, mirabegron, a beta-3-adrenergic agonist that acts specifically on the beta-3-adrenoreceptors in the wall of the bladder, has been developed. The drug relaxes the bladder wall during the filling and storage phase of micturition. Mirabegron was found in three separate randomized controlled clinical trials to significantly decrease urinary frequency and incontinence episodes, while significantly increasing bladder capacity (21). Although adverse effects are fewer than anticholinergics, patients may experience side effects such as hypertension, nasopharyngitis, urinary tract infection, and headache. Patients on mirabegron should have their blood pressure monitored and it is contraindicated in patients with uncontrolled hypertension. Anticholinergics have a high rate of discontinuation due to side effects: only 18% of patients continue with antimuscarinic medication after 6 months (21). Thus, pharmacotherapy is useful in cases of OAB but its effectiveness is limited due to side effects resulting in low patient compliance.Surgeries for incontinence
Overactive bladder
Intradetrusor botulinum toxin
Botulinum toxin is a presynaptic neuromuscular-blocking agent that causes selective and reversible muscle weakness.
The effect may last for several months when injected into the detrusor muscles (21): 100-300 units of the toxin, usually of the A subtype, are injected cystoscopically into the detrusor muscle at more than 10-15 different locations sparing the trigone. Postoperative urodynamic assessment usually results in significant increases in cystometric capacity of the bladder secondary to increased bladder wall compliance. There are reduced patient episodes of urgency and urgency incontinence; most patients report a reduction in requirement of antimuscarinic medications, some stopping these altogether. Patient satisfaction rates are high despite the increased incidence of voiding dysfunction and occasional urinary retention, the latter results in some patients needing to self-catheterize intermittently. Intradetrusor botulinum toxin is a safe option both in patients with neurogenic bladders and intractable OAB.Sacral nerve stimulation
Patients with OAB symptoms refractory to other less invasive methods may be offered sacral neuromodulation. Afferent sacral nerve fibres are activated (typically the S3 segment) which in turn inhibit parasympathetic motor neurons consequently preventing detrusor contractions. The procedure is often two-staged: in the first stage, the electrodes are tested to ascertain if the patient is likely to show an adequate response to stimulation (i.e. reduced number of voids or incontinence episodes). Up to 70% patients show a positive response and go on to have the second stage of the procedure, namely the permanent impulse generator implanted under the skin. Sacral nerve stimulation should be considered in refractory cases of OAB. About 10% of patients show no response and a smaller percentage need removal secondary to infection (21).
Percutaneous tibial nerve stimulation
Percutaneous tibial nerve stimulation (PTNS) is a minimally invasive, outpatient treatment with no major side effects that has been shown to decrease symptoms related to OAB.
PTNS involves placing a small needle electrode into the lower inner aspect of either leg near the medial malleolus. The electrode is connected to a stimulator that generates an electrical pulse, which then travels to the sacral nerve plexus via the tibial nerve. Similar to sacral neuromodulation, accessing the posterior tibial nerve stimulates sensory afferent nerves, but PTNS does so in a less invasive manner compared with direct sacral neuromodulation (19).Augmentation cystoplasty
This involves bivalving a functionally OAB and attaching a segment of intestine, usually ileum or sigmoid, to increase functional capacity and lower the end-filling pressure. Female patients are usually prone to infections in about 30% of cases; additionally, a significant proportion of patients may need to self-catheterize. It involves a major operation and should be used in only a selected group of patients. Advances in tissue engineering may offer a viable alternative to the use of bowel and this operation, as a result, may find a wider application in the future (19).
Suprapubic cystostomy
Intractable cases of OAB, especially patients with significant detrusor sphincter dyssynergia or neurogenic incontinence, who cannot, or find it difficult to void per urethram, may need to be offered a urinary diversion procedure such as a suprapubic cystostomy. In this procedure, a suprapubic catheter is inserted into the dome of the bladder usually under cystoscopic guidance. The catheter is then left in situ semipermanently. The catheter needs a change every 8-12 weeks, usually in clinic. In some patients it is possible to wean the patient off the catheter after and retrain them to void per urethram.
Stress urinary incontinence
• Retropubic bladder neck suspension
• Mid-urethral slings
• Urethral bulking agents (UBAs).
Retropubic bladder neck suspension
Principle: to reduce the hypermobility of the bladder neck thereby improving continence.
The procedure that is most commonly performed in the space of Retzius or the retropubic space is Burch colposuspension.
It used to be commonly performed via a transverse suprapubic incision such as a Pfannenstiel; however, for the past 20 years or more the procedure has been done laparoscopically as well. The procedure has lost its ‘sheen’ since the advent of mid-urethral slings in the 1990s, however it still has a role in women who either do not want a sling, are allergic to mesh, or are having a laparoscopic paravaginal repair for an associated cystocele, or indeed any concomitant laparoscopic procedure. The procedure involves the passage of two or three permanent or delayed absorbable sutures through the endopelvic fascia lateral to the mid urethra and bladder neck and then through the ipsilateral Cooper’s (iliopectineal) ligament and tied with gentle tension. Laparoscopic Burch colposuspension has been described using the transperitoneal or extraperitoneal approach. The extraperitoneal approach naturally minimizes the risk of intra-abdominal injury by avoiding intraperitoneal pelvic adhesions and is associated with a shorter learning curve. If patients are undergoing concomitant pelvic surgery, the transperitoneal approach may be more suitable (22); however, it tends to take longer. The advantages of laparoscopic pelvic surgery are better visualization, shorter hospital stay, better cosmetics, less postoperative pain, and faster recovery to normal daily activity. With open Burch colposuspensions, shortterm cure rates of 73- 92% have been reported; even after 5- 10 years, approximately 70% of patients are still continent. With laparoscopic Burch colposuspensions, the short-term cure rates are excellent, nearing 90%; however, the long-term cure rates are lower at about 59-68%. Urinary tract injury both to the bladder and ureter are commoner with laparoscopic Burch, as is the increased incidence of OAB, approximately 3-8% (22). Even in an era dominated by mid- urethral slings, laparoscopic Burch colposuspension does have a niche role in the management of SUI.Mid-urethral synthetic slings
Principle: to improve continence by enhancing support to the mid urethra.
The hammock theory by DeLancey urethral support is provided by the layers outside the urethra on which it rests (23):
• The anterior vaginal wall
• The endopelvic fascia between the arcus tendineus fascia pelvis on each side
• Pelvic floor muscles (Figure 57.4).
When this ‘shelf’ oftissue is intact, any increase in intra- abdominal pressures causes the urethra to remain shut against it. It is when this shelf is injured during childbirth or atrophied with age and consequent hypo-oestrogenism that urethral hypermobility and/or SUI may result. In fact, in patients with a mid- urethral sling, stress causes a dynamic kinking of the urethra against the resistance provided by the shelf of tissue, thus preventing stress leakage (24).
Since the introduction of mid-urethral slings in the 1995 by Ulmsten based on the ‘integral theory of female urinary continence’ by Petros and Ulmsten (25), the focus of continence surgery shifted Retropubic slings The original tension-free vaginal tape (TVT) procedure placed a polypropylene sling at the level of the mid urethra via a ‘bottom-to-top’ approach. This is still the preferred approach and the GYNECARE TVT EXACT Continence System (Ethicon, USA), is a popular product exemplifying this technique. The trocar attached to the sling is passed from a mid-urethral vaginal incision through the para-urethral tunnels in the endopelvic fascia and the retropubic space to a suprapubic exit point, one on each side of the midline. The ‘top- to-bottom’ technique was developed in 2001 (26) with the introduction of the Suprapubic Arc system (SPARC, American Medical Systems, Inc., Minnetonka, MN, USA) sling. This technique involves passage of the trocar from a suprapubic incision through all of the above-mentioned layers to a suburethral incision. Regardless of the type of approach, the procedure involves careful identification of mid urethra—a failure to do so may result in the sling being sited close to the bladder neck, predisposing the patient to develop postoperative voiding dysfunction. Most importantly the sling is placed ‘tension free’: if the sling is placed too tight, there is a potential for postoperative voiding problems that manifest commonly as a failed trial of void, that is, the inability of the patient to pass urine per urethram immediately after surgery, or more rarely, as urinary retention or overflow incontinence. Occasionally, the patient needs to return to theatre and the tape may have to be loosened/ divided. Interestingly, division of the tape does not lead to failure of
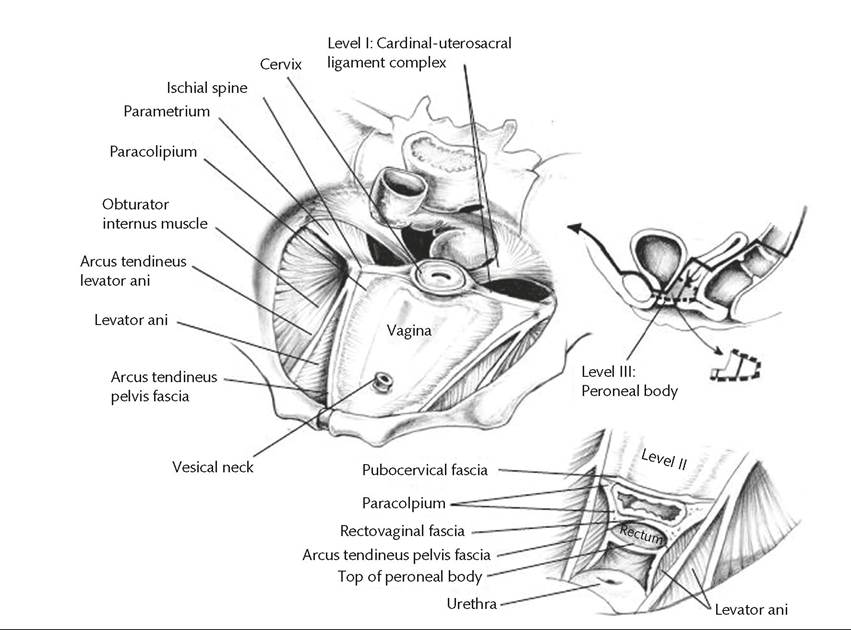
Figure 57.4 DeLancey's levels of support.
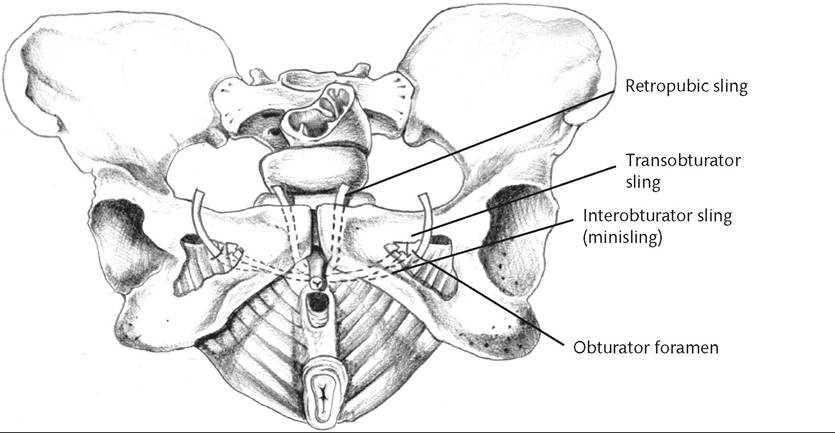
Figure 57.5 Types of mid-urethral slings and their trajectories.
the procedure as 80% of the patients still remain continent. Hence all patients have a strict ‘trial of void' protocol in the first 2-3 hours postoperatively. During this time, patients are given only enough fluid to fill their bladders comfortably enough for them to void spontaneously. A bladder scan is done after voiding to look at residuals. As a rule of thumb, if the patient voids 200-300 mL of urine and has less than this in her bladder on scan, she is deemed to have passed a trial of void. A lot of other factors such as pain, postoperative swelling, associated prolapse surgery, a ‘tight sling' (see earlier in this paragraph), and unfamiliar surroundings may impact the patient's ability to void successfully postoperatively. Therelore, patients are given adequate pain relief preferably with anti-inflammatories, prescribed aperients and sent home to more familiar environs. Postoperative voiding difficulty after a mid-urethral sling procedure is an unfortunate but well-known temporary complication of pelvic surgery with an occurrence of approximately 3-10% (27).
Transobturator slings The next generation of mid-urethral slings were the transobturator tape (TOT) slings. The vaginal incision is still very similar to the one described in the previous section and is usually smaller. The double helix needle is inserted through a stab incision in skin overlying the obturator foramen just below the insertion of the adductor longus tendon. The needle is then driven through the obturator fossa to exit via the through the para-urethral tunnels created via the vaginal incision up to the level of inferior pubic ramus. The polypropylene sling is then attached to the needle tip and withdrawn through the track described above to exit at the obturator incision. The original TOT operation was described as an ‘outside-in' technique with the tape being passed from the thigh into the vaginal incision (Uratape, PorgesMentor, Le Plessis, Robinson, France & Monarc, AMS, MN, USA). The technique was later modified as an ‘inside-out', approach, with a vaginal incision through the obturator foramen and out through the inner thigh as the TVT-Obturator system (TVT-O, Ethicon Inc., Johnson & Johnson, Somerville, NJ, USA) (28). As with the TVT, the sling should be sited in a tension-free manner well away from the bladder neck. Trial of void protocols are similar. Postoperative voiding dysfunction is lower with TOT when compared to TVT.
Single-incision minislings The latest entrants to the sling ‘market' are the single-incision minislings (SIMS). These slings require a vaginal incision similar to the one described previously and involves creation of the para- urethral tunnels to the inferior pubic ramus. The obturator membrane is then ‘perforated' with the tip of the scissors to facilitate the passage of the sling needle. The SIMS needle with the polypropylene sling loaded to its tip is inserted via the para-urethral tunnel on the patient's left through the perforation in the obturator membrane and inserted into the obturator internus muscle to which it remains anchored. The procedure is repeated on the patient's right, this time however, the sling is released from the needle only after it is appropriately ‘tensioned' under the urethra. Thus the SIMS differs from the TVT and TOT in that it is not ‘tension free', in fact, it is quite the opposite. Despite this, the rates of postoperative voiding dysfunction are no different to that with the other two slings.
Type 1, macroporous, monofilament polypropylene mesh is used for all types of slings. The type 1 mesh promotes prompt ingress of fibrous connective tissue and capillaries thus encouraging tissue host ingrowth and integration allowing the mesh to anchor within the tissue. This inflammatory response wanes with time thus reducing the risk of infection (28).
Indications
1. Urodynamic SUI
2. Low-pressure (low maximum urethral closure pressure/Valsalva leak point pressure) SUI (intrinsic sphincter deficiency)
3. (Selected cases) of MUI.
Although the classical indication for slings is patients with urethral hypermobility, slings are also being increasingly used in patients with intrinsic sphincter deficiency who typically get offered UBAs.
Studies comparing TVT, TOT, and SIMS Cure with mid-urethral slings is described in ‘objective' or ‘subjective' terms. Objective cure is the absence of SUI on a cough test usually in the context of a postoperative urodynamic assessment. Subjective success is the patient's perception of improvement measured via validated questionnaires such as the Patient Global Impression of Improvement (PGI-I) and Incontinence Quality of Life Questionnaire (I-QOL). Slings have been extensively studied over the past 20 years and there are numerous studies that provide a large amount of good quality (level 1 and 2 evidence) that support the concept of a sling placed at the level of the mid urethra. Long-term follow-up has been published for the original TVT procedure with the most recent publication (28) providing level 2 evidence with mean follow-up of 11.5 years (of 77% of patients from the original series published by Nillson et al.), revealing an objective cure was found in 90% of women and subjective cure in 77%, based on the PGI-I. With TOT, studies have quoted mid-term (i.e. 3-5-year) cure rates of 82.4-88.4% (28). High-quality data indicate about a 7-10% failure rate for both the transobturator and the retropubic approaches, with comparable short-term cure rates.
In a 3-year follow-up by Basu and Duckett, there was a significantly higher 3-year failure rate for a SIMS versus a retropubic mid- urethral sling (29). Both procedures had reduced efficacy over time. Another multicentre trial published in 2014 indicated that SIMS has no advantage in terms of safety over TVTs and was found to be less effective than TVTs (30). Other studies, however, indicate otherwise. A meta-analysis published in 2014 showed that there was no evidence of significant differences in patient-reported and objective cure between currently used SIMS and other slings at mid-term follow-up and SIMS were associated with more favourable recovery time (31). A more recent meta-analysis shows no significant difference in the patient-reported cure rate and objective cure rate between SIMS and TOT (32).
Comparison of slings with other procedures for SUI In a high- quality, multicentre randomized controlled trial of TVT versus Burch colposuspension, the authors showed equivalent efficacy of cure for TVT and Burch colposuspension in a 5-year follow-up (33). There was no difference in success in a 1-hour stress pad test (81% vs 90%), stress leakage (63% vs 70%), or satisfaction rates (91% vs 90%). Hospital stay was significantly shorter for the TVT group and there was no difference in the chance of reoperation, although patients who had colposuspension were more likely to require prolapse surgery. TVT was more cost-effective than Burch colposuspension. The Cochrane review found that slings (TVT) had a shorter operating time (35 vs 87 minutes) and shorter hospital stays (34). For open colposuspension versus slings, objective cure rates at 12 months were 79% for synthetic slings versus 82% for colposuspension. For laparoscopic colposuspension versus slings, no significant difference in patient-reported outcomes within 12 months was shown; 80% for slings versus 74% for colposuspension (34).
Urethral bulking agents
UBAs are injectable materials used as a minimally invasive way to treat intrinsic sphincter deficiency by increasing the urethral closure pressure and thus increasing resistance to urinary flow. These agents are also viable alternatives for patients who have failed other options such as slings, who desire a less invasive option, those who pose an anaesthetic risk, those with a fixed scarred urethra, and women of childbearing age who desire more children (35). UBAs are composed of either biological (collagen, autologous fat) or synthetic materials (silicone, polyacrylamide hydrogel, carbon beads, calcium derivatives) that are injected transurethrally via a cystoscope into the mid urethra. The biological agents assimilate into tissues over time and therefore patients need reinjections to maintain ongoing symptomatic benefit. For synthetic agents, however, reinjection is not often required—they are therefore generally more effective (35). Macroplastique, Durasphere, Coaptite, Bulkamid (all synthetic), and Contigen and Collagen (biological) are some examples of UBAs. In patients who underwent UBA injection with Macroplastique, substantial durable results were obtained during 2 years with 84% of patients dry at 1 year, and two-thirds at 24 months (36). Three studies meeting the inclusion criteria were identified. Three randomized controlled trials evaluating the use of UBAs versus other surgical procedures for the treatment of female SUI showed that the objective recurrence rate of peri- or transurethral injections is significantly higher in comparison with the other surgical procedures in the treatment of primary or recurrent SUI. However, the incidence of voiding dysfunction is lower with UBAs. In summary, UBAs should not be proposed as first-line treatment in those women seeking permanent cure for both primary and recurrent SUI. However, the effectiveness of a procedure should be balanced with its invasiveness and patients' expectations, where UBAs have a definite role (37).
More on the topic Management of incontinence:
- Faecal incontinence
- Chapter 30 Pelvic Support Defects, Urinary Incontinence, and Urinary Tract Infection
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Management of perineal trauma
- Management of gastrointestinal symptoms
- Evaluation of female urinary incontinence
- The practice of obstetrics and gynecology encompasses a broad spectrum of care directed to many aspects of a woman’s health (see also Appendix J).
- Management of pelvic organ prolapse
- Chapter 15 Common gynaecological procedures and surgery
- CONTENTS