External cephalic version
A brief history of ECV
ECV has been described in the medical literature since the writings of Hippocrates (around the fourth century âńĺ) to convert a breech presenting pregnancy to a cephalic presenting one.
It did not gain popularity until the beginning of the nineteenth century. However, in the early twentieth century, ECV was often performed in preterm gestation under general anaesthesia and it was associated with high perinatal mortality. That meant that the procedure of ECV was almost abandoned. Since the 1980s, ECV has been revived, due to the assistance of ultrasound surveillance and effective uterine relaxation by tocolytic agents. Both these adjuncts have made ECV a very safe procedure with a high success rate in current obstetric practice.Indications of ECV
Breech presentation is the most common indication for ECV. ECV may be considered in cases of unstable lie and transverse or oblique lie, provided there is no contracted pelvis or other contraindication to have ECV and vaginal birth has been ruled out. In the cases of abnormal lies, induction of labour immediately after a successful ECV may help to minimize the chance of reverting to abnormal lie.
Contraindications for ECV
Absolute contraindications are few and include conditions where CS is required even if the fetus is in cephalic presentation (such as placenta praevia and contracted pelvis), or there are known structural uterine anomalies (congenital or lower segment fibroids) causing malpresentation or abnormal lie, or the fetal well-being is already compromised (evidenced by an abnormal CTG trace). The umbilical cord tightly wound around the fetal neck, ruptured membranes, or a recent history of antepartum haemorrhage (within 7 days) are also contraindications for ECV.
ECV may be relatively contraindicated if the estimated chance of successful ECV or successful vaginal delivery is low, or if the procedure might be more complicated, such as oligohydramnios, a small-for gestational-age fetus with abnormal Doppler parameters, major fetal anomalies, a scarred uterus, or pre-eclampsia is present (20).
Procedure of ECV
Preoperative preparation
Pre-ECV assessment is an important safeguard of the procedure. First of all, any doubts in gestational age need to be resolved before ECV, as the procedure should not be done prior to 36-37 weeks of gestation, when there is still a good chance of spontaneous cephalic version. Furthermore, if the pro cedure is complicated, it may result in an iatrogenic preterm delivery. Rhesus-negative mothers must have prophylactic rhesus antibodies immediately after ECV to prevent rhesus isoimmunization. Crossmatching blood and an intravenous line access should be prepared in case emergency CS is required after a complicated ECV. Performing ECV in the labour ward or in a site close to labour ward is preferred. Beta-sympathomimetic tocolytics are contraindicated in maternal cardiac or thyroid disorders which should be ruled out. Ultrasonography and CTG should be performed to rule out any contraindications for ECV. Furthermore, ultrasonography will help to assess the position of the fetal spine and that of the placenta, both of which are important factors for planning the direction of the version.
The turning procedure
The operator firstly has to decide the direction of turning, which will depend on the placenta site and the position of the fetal back. It is important to avoid going against the placenta. If a clockwise direction is decided, the operator should stand on the maternal left side so that he/she will push the fetal breech to the contralateral side (and vice versa). ECV should only be attempted when the uterus is relaxed. Short-acting tocolytics (such as terbutaline and hexoprenaline) are useful to relax the uterus. They may cause palpitation and occasionally induce significant hypotension. Prophylactic fluid loading through an intravenous line may be considered.
If the fetal breech is engaged in the maternal pelvis, a gentle force is needed to elevate it from the pelvis. The breech is then pushed (using the operator’s thumbs) to the iliac fossa on the other side.
Once it is successful, the breech is maintained in this location by one of the operator’s hand. The operator then uses the other hand to pull the fetal head to the cornual region close to himself/ herself. Once the fetus is in oblique lie and both the fetal poles are under the control of the operator’s hands, the operator can further rotate the fetus to transverse lie by simultaneous forces on both fetal poles. Once the fetal lie becomes transverse, cephalic version can usually be completed in majority of the cases. Forceful or jerky movements should always be avoided. The procedure usually takes about a few seconds to 10 seconds, and seldom more than 20 seconds. If an attempt is failed, the operator may try again but not more than three times.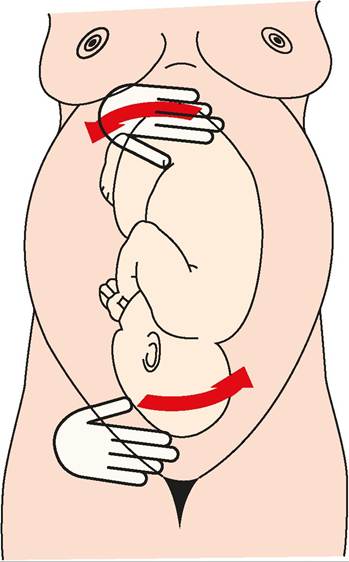
Figure 33.7 The procedure of external cephalic version.
Anaesthesia
In general, ECV is performed without any anaesthesia, which would block a woman's pain sensation and hence unfasten the safeguard against forceful movements of an inexperienced operator. However, recent studies have shown that spinal anaesthesia may relax the maternal abdomen, reduce the force of version, and improve the success rate in experienced hands (21, 22).
Postoperative assessment
After an ECV, the fetal heart rate should be counted immediately with real-time ultrasound to rule out any bradycardia. Transient decelerations are common (3-5%) and should not last for more than 2 minutes. It is often a physiological reaction towards pressure exerted on it (in particular on its head) (23). However, when there is persistent bradycardia, an emergency CS should be considered to minimize fetal risk.
If there is no immediate fetal heart rate disturbance, the fetus should be monitored with CTG for another 30-60 minutes before the patient can be discharged home safely. Any symptoms of rupture of membranes, antepartum haemorrhage, or abdominal pain should be further investigated and managed accordingly.
After a successful ECV, the patient should be followed up a week later to rule out any reversion to breech presentation. If not, then the patient can be managed as other spontaneous cephalic presenting cases, understanding that the risk of intrapartum CS after successful ECV is still higher than that of spontaneous cephalic presenting pregnant women.
Risks and complications of ECV
Major complications of ECV are uncommon (24). Transient fetal bradycardia (3800 g).
• A growth-restricted baby (usually defined as in a flexed position during the decent of the fetal head is crucial for a smooth delivery. This can be facilitated by the following two common methods:
Mauriceau-Smellie-Veit manoeuvre
In this manoeuvre, the fetal chest and abdomen is first placed on the operator’s left palm and forearm, with the fetal legs straddled over the operator’s forearm. The operator’s left index and middle fingers are inserted into the vagina to identify the fetal maxillas, one on each side. The operator’s right index finger and fourth finger are then put over both fetal shoulders, one on each side, to exert a downward traction. The fetal head flexion is facilitated by the simultaneous exertion of force on the maxillas by the left index and middle fingers, and on the occiput by the right middle finger (Figure 33.9). Care should be taken to avoid blindly pressing the left fingers on the fetal eyeballs (just above the maxillas), or inserting the fingers into the fetal mouth and to pull the lower jaw. Suprapubic pressure by an assistant may help to facilitate the fetal head flexion. The fetal body is then elevated towards the maternal abdomen, so that the fetal head gradually rotates out of the perineum starting from the fetal mouth, nose, brow, and eventually the occiput.
Forceps to aftercoming head
Grasping the fetal head with a pair of forceps properly can ensure the head flexion during the descent process. Piper’s forceps are designed specifically for such a purpose (Figure 33.3).
In contrast to cephalic forceps delivery, Piper’s forceps should be inserted from below the level of the fetal body (Figure 33.10), and it is more easily done when the operator kneels down. Secondly, the Piper’s forceps should be held horizontally with their shanks parallel to the perineum at the beginning of insertion. With the fetal head in the OA position, the blades are slid into the vagina, one after the other, in a similar manner as in cephalic forceps delivery. After successful locking of the forceps, the fetal head is pulled out by the blades while the shanks and handles are swung upwards to deliver the fetal head in the flexed position.Burns-Marshall method
The fetal feet are grasped and with gentle traction they are swept over the maternal abdomen, and sometimes the delivery of the fetal head may follow in simple cases. However, unlike the Mauriceau- Smellie-Veit manoeuvre or forceps delivery, the Burns-Marshall
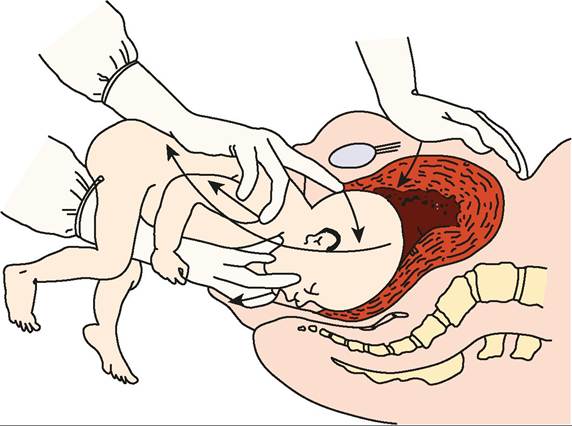
Figure 33.9 The Mauriceau-Smellie-Veit manoeuvre.
method does not promote fetal head flexion, and hence may not help to relieve the aftercoming head. There is also concern about the risks of the Burns-Marshall method if used incorrectly, leading to overextension of the baby's neck.
Risks and complications of assisted vaginal breech delivery
One of the major risks of vaginal breech delivery is fetal hypoxic injury, as the umbilical cord is vulnerable to compression or vasoconstriction once it is outside the cervix during the delivery process. Delayed delivery caused by nuchal arm or head entrapment increases the risk of hypoxia. Birth trauma such as fractures, nerve injury, and visceral injury can be caused by forceful traction or poor manipulation by inexperienced hands. A recent meta-analysis shows that although planned vaginal delivery is associated with a two to five times higher perinatal complication rate than planned caesarean delivery, its absolute mortality (0.3%), neurological morbidity (0.7%), and birth trauma rate (0.7%) remain at a low level that keep it a viable option in selected cases (28).