Fetoscopic procedures
The term fetoscopy is used to describe the endoscopic visualization of the fetus (41). Today, therapeutic fetoscopy has several indications including laser ablation for TTTS, selective reduction of monochorionic twin pregnancies, and endotracheal occlusion in the prenatal management of congenital diaphragmatic hernia (CDH).
Fetoscopic laser ablation for twin-to twin transfusion syndrome
TTTS arises in approximately 10% of monochorionic twin pregnancies between 16 and 26 weeks’ gestation (42). This condition occurs in a previable period, the prognosis is therefore extremely poor and mortality approaches 90% without treatment. Sonographic diagnosis of TTTS is characterized by an amniotic fluid discordance, that is, polyhydramnios and a distended bladder in the volume- overloaded recipient and oligohydramnios and a small or empty bladder in the volume-depleted donor. The pathophysiology of this condition is thought to be secondary to an imbalance in blood flow across placental anastomoses. In 1999, Quintero et al. developed a staging classification system for TTTS after evaluating the prognostic value of sonographic and clinical parameters (43). The limitations of this staging system are associated with the fact that the disease evolution of TTTS is unpredictable. Prior to the introduction of fetoscopic laser coagulation, serial amnioreduction was the mainstay of treatment for TTTS. In 2004, a randomized controlled trial compared the safety and efficacy of endoscopic laser surgery to serial amnioreduction in the treatment of severe TTTS and demonstrated that the perinatal outcomes were significantly better in the laser group (44). The procedure is typically performed with maternal anxiolysis and local anaesthetic. Under ultrasound guidance, a trocar is advanced into the gestational sac of the recipient twin. Endoscopes with diameters of 1-3 mm are available and uterine distension with normal or physiological saline may occasionally be used to improve visualization.
Laser photocoagulation of the communicating vessels is performed (Figure 19.3 and ©Video 19.2) and surgery is completed following amniodrainage of the recipient’s sac.Several modifications of the laser technique including selective and sequential selective laser coagulation have been described since the original description of coagulation of all vessels crossing the inter-twin membrane. The Solomon technique involves coagulation of the entire vascular equator from one placental margin to the other, with the aim of reducing the number of residual anastomoses and hence the associated complications of twin anaemia-polycythaemia sequence, or recurrent TTTS. A subsequent trial reported that this method reduces associated postoperative fetal morbidity and recommended that fetoscopic surgeons consider incorporating this technique into their own practice (45). Although fetoscopic laser coagulation is a safe and effective procedure for the management of
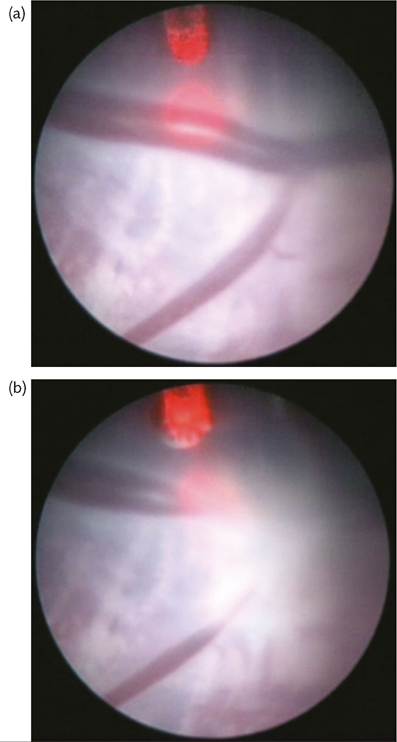
Figure 19.3 Vascular anastomoses during fetoscopic laser treatment of TTTS-(a) before and (b) after photocoagulation.
severe TTTS, it is associated with complications. The survival rates of both fetuses have improved significantly to approach over 70%. Significant complications relating to the procedure include iatrogenic PPROM, twin anaemia-polycythaemia sequence, recurrence of TTTS, and adverse long-term neurological sequelae in 6-18% of survivors (46). The future of fetoscopic laser therapy in the treatment of TTTS will involve evaluating its role in the management of early disease—a randomized controlled trial is currently underway to compare conservative management to laser therapy for the treatment of TTTS stage 1.
Fetoscopic cord occlusion for selective fetal growth restriction or discordant fetal anomaly in monochorionic twin pregnancies
Selective fetal growth restriction affects 12-15% of monochorionic twin pregnancies (47).
Isolated selective fetal growth restriction is usually defined as an inter-twin size difference of 25% or greater in the absence of TTTS and is easily differentiated from TTTS due to a lack of polyhydramnios surrounding the appropriately grown fetus. There is also an increased incidence of discordance in fetal anomalies in monochorionic twin pregnancies compared to dichorionic pairs. This is most likely due to the teratogenic effect of embryo cleavage or as a result of shared circulation. Either of these conditions may lead to intrauterine demise of one twin and potential neurological injury to the other. In certain situations, selective feticide of one twin is offered to maximize the chances of survival of the co-twin. As a consequence of shared placental circulation, selective termination is achieved by interrupting the vascular supply of the affected twin. This may be achieved by bipolar cord coagulation, cord ligation, ILT, or RFA.Fetoscopic cord coagulation requires the insertion of a 3.8 mm operative sleeve into the amniotic sac of the fetus that is to be terminated (48). Sufficient amniotic fluid is required to facilitate insertion of the sleeve and deployment of the device. Complications associated with fetoscopic cord occlusion include membrane rupture, preterm labour, and haemorrhage. Intrauterine demise of the co-twin has been reported in up to 15% of cases (49). Bebbington et al. performed a retrospective review of the outcomes associated with selective termination by bipolar cord coagulation compared to RFA. The overall survival rates of the co-twin associated with bipolar cord coagulation versus RFA were 85.2% and 70.7% respectively (48). The increased overall survival in the bipolar cord coagulation group was attributed to decreased time taken to achieve cessation of blood flow. The optimal therapeutic technique to achieve selective reduction in monochorionic twin pregnancies is yet to be defined.
Fetoscopic endotracheal occlusion for congenital diaphragmatic hernia
CDH is a defect of the diaphragmatic wall which results in protrusion of the abdominal organs into the thoracic cavity.
It affects approximately 1 in 4000 live births and is associated with a chromosomal abnormality in 30% of cases (50). Cases of isolated CDH are associated with a 50% mortality rate secondary to pulmonary hypoplasia and hypertension. Over the years, studies have recognized predictors of outcome for CDH including gestational age, additional anomalies, herniation of the liver, and the measurement of the observed to expected fetal lung area to head circumference ratio (51). The concept of intrauterine repair to replace the herniated viscera and subsequently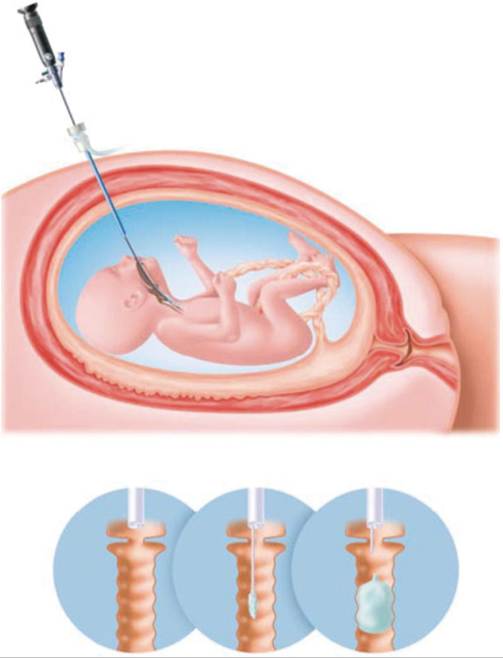
Figure 19.4 Schematic drawing of fetoscopic endoluminal tracheal occlusion using a detachable balloon.
Reproduced from J. Deprest, E. Gratacos, K. H. Nicolaides, Fetoscopic tracheal occlusion (FETO) for severe congenital diaphragmatic hernia: evolution of a technique and preliminary results, Ultrasound in Obstetrics and Gynaecology, Vol 24 No 2, August 2004, with permission from John Wiley and Sons.
reverse the effects of pulmonary hypoplasia and pulmonary hypertension were first demonstrated in animal studies. These were abandoned, however, as the procedure was associated with high rates of maternal morbidity and did not confer any significant improvement in neonatal mortality or morbidity (52). Endotracheal occlusion in humans was originally performed via open hysterotomy and subsequently endoscopically by means of tracheal clip application. The removal of these clips required a strict delivery protocol which gave rise to the EXIT procedure. As a consequence of increased rates of preterm delivery and irreversible damage to the trachea, clips were subsequently abandoned in favour of endotracheal balloon occlusion (Figure 19.4). In 1999, a prospective randomized controlled trial of fetal endotracheal occlusion versus standard postnatal care for fetuses with severe isolated left CDH was terminated early after treatment of 24 patients failed to demonstrate a significant benefit in outcome (53).
Failure to demonstrate a significant difference in survival to 90 days may be explained by the fact that the fetuses in the interventional group were born at significantly earlier gestations than those in the control group.Following on from this trial, numerous centres have been involved in the development of endoscopic techniques (fetoscopic endotracheal occlusion) and protocols to tackle the significant complication rate associated with CDH. A case series of 210 procedures reported a substantial increase in survival for both left- and rightsided severe cases of CDH treated with fetoscopic endotracheal occlusion. PPROM complicated 47% of these cases and 7 of the 210 mothers experienced a procedure-related complication (54). Fetoscopic endotracheal occlusion has demonstrated the potential to improve survival rates and reduce the morbidity of fetuses with suspected severe pulmonary hypoplasia secondary to CDH. It remains to be an investigational procedure, however, rather than standard therapy. Ongoing research into its application in cases with suspected moderate hypoplasia as well as the long-term outcomes of survivors remain key issues that need to be addressed.