Ultrasound-guided fetal therapy
Some of the first ultrasound images of the fetus were published in The Lancet by Donald et al. in 1958 (15). Over the last 60 years, technological advances have included real-time imaging, colour and power Doppler, transvaginal sonography, and three/four- dimensional imaging.
Ultrasound-guided techniques including intrauterine blood transfusion (IUT), direct fetal pharmacological therapy, radiofrequency ablation (RFA), interstitial laser therapy (ILT), selective fetal reduction, and shunting procedures constitute an essential part of fetal therapy.Intrauterine blood transfusion
Rodeck et al. described the technique of intravascular IUT into the umbilical cord under fetoscopic guidance (16). Despite widespread use of anti-D immunoglobulin, IUT under ultrasound guidance remains the definitive treatment for fetal anaemia secondary to red cell alloimmunization. It has also been described in the management of fetal anaemia secondary to non-immune conditions such as parvovirus, twin-to-twin transfusion syndrome (TTTS), fetomaternal haemorrhage, and placental chorioangioma. Invasive techniques such as amniocentesis and fetal blood sampling were previously used to diagnose fetal anaemia in utero. These procedures, however, carry an increased risk of miscarriage, preterm labour, and fetal loss. Today, measurement of the peak systolic velocity in the middle cerebral artery is the standard non-invasive screening technique for fetal anaemia (17). When performing IUT, access to the fetal circulation is via the umbilical cord typically at the placental cord insertion site (Figure 19.1 and Q Video 19.1). The umbilical vein is chosen preferentially as it has a wider diameter and is also less likely to spasm than the umbilical artery. Under circumstances where the umbilical vein is inaccessible (e.g. posterior placenta or advanced gestation), the intrahepatic portion of the umbilical vein or a free loop of umbilical cord may be used as an alternative.
Intravascular transfusion into a free-floating loop of umbilical cord is associated with an increased risk of displacement, cord tamponade, and higher fetal loss rate (18). Prior to 20 weeks' gestation, the intraperitoneal route remains the method of choice, where the donor red cells are absorbed into the fetal circulation via the lymphatic system. The intracardiac route via the apex of the left ventricle has also been described in the literature (19). This technique, however, is associated with an increased risk of cardiac tamponade and fetal arrhythmias.The need for serial IUTs is dependent on the gestation of the first procedure and the severity of fetal anaemia. Monitoring via the middle cerebral artery peak systolic velocity may guide the need for a repeat procedure. This would typically be performed 2-3 weeks following the first transfusion. The interval following the second transfusion is more predictable, however, as the red cells in the fetal circulation are almost exclusively adult and therefore fetal erythropoiesis is suppressed. The fall in the haematocrit is 1% per day due to plasma expansion and fetal growth rather than haemolysis. The

Figure 19.1 Intrauterine transfusion.
interval between the second and third procedure is typically 3-4 weeks. Given the associated risks with this procedure, delivery rather than repeat IUT after 35 weeks is the preferred management strategy. Despite survival rates of greater than 90%, IUT has associated procedure-related complications including fetomaternal haemorrhage, fetal heart rate abnormalities, chorioamnionitis, cord accidents, volume overload, preterm prelabour rupture of membranes (PPROM), and preterm labour. Procedure-related fetal loss rates vary in the literature from 0.9% to 4.9% per procedure and are associated with hydrops, severity of anaemia, early gestational age, transfusion into a free loop of umbilical cord, and the experience of the operator (20).
Following delivery, these neonates tend to require more top-up transfusions in the first 6 months of life. Small fetomaternal haemorrhages which occur at the time of IUT, particularly during transplacental puncture, may cause increased sensitization in the current and future pregnancies.Direct fetal pharmacological therapy
In cases of failed transplacental therapy for the treatment of fetal arrhythmias, direct fetal therapy has been described. This is largely indicated as a measure of last resort in cases of very preterm or hydropic fetuses in which delivery would be inappropriate. Direct therapy may be achieved by intravenous (IV) infusion of an antiarrhythmic drug into the umbilical vein. The technique for performing this procedure would be similar to that for IUT. More rarely, fetal intramuscular (IM) injection may be undertaken under ultrasound guidance. Infusion of digoxin, amiodarone, verapamil, and adenosine via IV or IM routes have all been described in the literature (21, 22).
Radiofrequency ablation
RFA occurs when radiofrequency waves passed through tissue cause an increase in tissue temperature. The application of percutaneous RFA in obstetrics has been reported mostly in the management of twin reversed arterial perfusion (TRAP) sequence and sacrococcygeal teratoma (SCT). TRAP sequence is a rare complication exclusive to monochorionic twin pregnancy in which one twin (acardiac) with varying degree of anomalous cardiac structure is dependent on the circulation of the normal (pump) fetus (23). Placental anastomoses allow blood to flow from the umbilical artery of the healthy pump twin in a reversed direction into the umbilical artery of the acardiac fetus. The clinical consequences for the healthy fetus include cardiac failure and polyhydramnios resulting in preterm delivery. If untreated mortality rates as high as 55% have been reported (24). Previous treatment options have incorporated cord occlusion of the acardiac twin and amnio drainage.
Over the last decade, ablative therapies such as RFA have been used to interrupt the vascularization of the acardiac twin.Fetal SCT is a rare neoplasm, which complicates approximately 12 per 20,000 pregnancies (25). Due to improved antenatal detection, the frequency of diagnosis is increasing. Perinatal mortality rates of prenatally diagnosed SCTs range from 25% to 37% (26). Fetuses with solid, rapidly enlarging, highly vascularized teratomas can develop high-output cardiac failure and non-immune hydrops via vascular shunting. Observational studies have determined that SCTs associated with cardiac failure and fetal hydrops have a mortality rate which approaches 100%. If cardiac failure occurs following viability, early delivery, possibly with ex utero intrapartum treatment (EXIT) and postnatal surgery, may be the best management strategy. Prior to viability, therapeutic techniques including open fetal surgical resection and percutaneous coagulation such as RFA to decrease vascular shunting have rarely been described.
RFA is typically carried out under maternal anxiolysis and local anaesthesia. The ablation system is a monopolar device and therefore grounding pads are applied to the maternal skin to complete the circuit. The needle electrode is inserted percutaneously under ultrasound guidance, for example, in TRAP sequence this would typically be adjacent to the umbilical cord insertion of the acardiac twin. Colour Doppler ultrasound can be used during the procedure to demonstrate cessation of flow within the umbilical artery or the vascular supply to the teratoma. An ultrasound scan should be performed 12-24 hours following the procedure to ensure cessation of blood flow. The most common postprocedure complication is PPROM. Cabassa et al. performed a systematic review of twin pregnancies complicated by TRAP sequence managed with RFA. In 78 pregnancies there was an 85% neonatal survival rate with 22% of the treated pregnancies complicated by PPROM and two reports of maternal thermal injury (23).
In hydropic SCT fetuses undergoing interstitial laser or RFA, survival was found to be 45% with the major associated complications being PPROM and associated preterm delivery (26). Despite small numbers and in the absence of long-term outcomes, RFA appears to be a relatively safe and effective procedure in the management of twin pregnancies complicated by TRAP sequence and prenatal treatment of fetal SCT.Interstitial laser therapy
ILT uses an image-guided needle to deliver laser energy into a tumour to heat and destroy the abnormal cells. ILT has been described in the management of fetal SCT and chorioangioma. Chorioangioma are vascular lesions present in approximately 1% of placentae. Giant chorioangiomas (>4 cm in diameter) have a prevalence of 1 in 9000 pregnancies and are associated with a range of fetal complications including anaemia, polyhydramnios, hyperdynamic heart strain, hydrops, growth restriction, and fetal demise in up to 30% of cases (27). Treatment options in early pregnancy include amniodrainage to alleviate polyhydramnios and IUT in the presence of fetal anaemia. These procedures provide symptomatic relief but do not treat the underlying cause. A variety of techniques including ILT have been proposed to ablate the vascular supply to the tumour. The 17-18 G ILT needle is positioned under ultrasound guidance and a 400-600-micron laser fibre is advanced a few millimetres from the tip of the needle into the target tissue (Figure 19.2a). Power is applied until the tissue close to the fibre becomes echogenic and the blood flow ceases (Figure 19.2b) (28). Zanardini et al. published the results of a retrospective analysis of 19 cases of pregnancy complicated by antenatally detected placental chorioangioma. Eighteen of the nineteen cases were associated with a fetal complication. ILT was performed in three cases under ultrasound guidance to devascularize the tumour and prevent the development of fetal hydrops and associated compromise.
All three cases were associated with a successful pregnancy outcome (27). The advantages of ILT include the ability to perform this minimally invasive technique under local anaesthetic and that it is technically easier compared to endoscopic laser coagulation (27).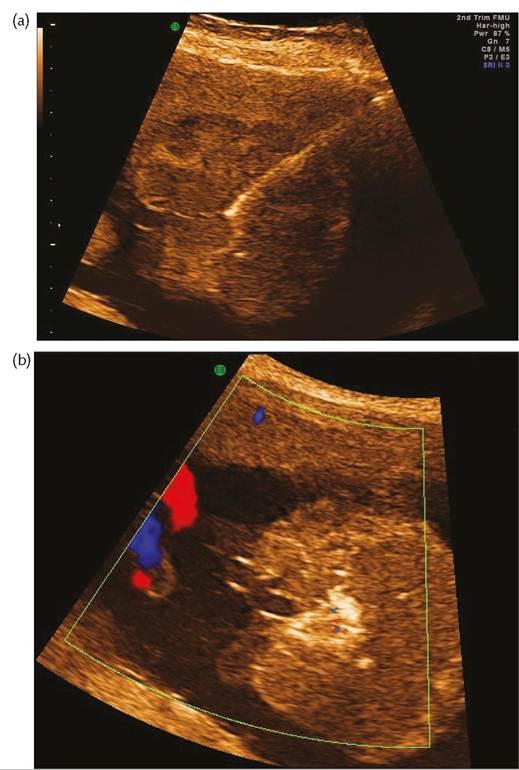
Figure 19.2 (a) Insertion of an 18 G ILT needle under ultrasound guidance into a giant placental chorioangioma. (b) Echogenic tissue adjacent to ILT laser fibre during treatment of the same placental chorioangioma as in (a).
Selective fetal reduction-dichorionic twin pregnancies
While the true incidence of structural anomalies in twin pregnancies is difficult to determine, approximately 2-3% of dizygotic twins are thought to be affected. This is similar to that of singleton pregnancies; however, the risk is increased two- to threefold in monozygotic pairs (29). Dichorionic twin pregnancies lack placental anastomoses and, as such, the passage of substances from one twin into the circulation of the co-twin is unlikely. Selective fetal reduction in dichorionic twin pregnancies that are discordant for anomaly can therefore be performed safely by injection of a drug that will induce asystole in the affected fetus. Injection of potassium chloride into the fetal heart or less frequently the umbilical vein under ultrasound guidance is an established technique. A key principle of this procedure is the importance of meticulous fetal labelling (30). This is particularly relevant in dichorionic pregnancies with concordant gender and minor abnormalities. Following a detailed ultrasound scan the affected fetus is identified. Using aseptic technique and ultrasound guidance, typically a 20-22 G needle is inserted through the maternal abdomen into the left ventricle and if intracardiac access is not possible, the umbilical vein may be used. A retrospective analysis of 106 fetocide procedures concluded that both intracardiac and umbilical routes may be used to achieve feticide effectively without compromising maternal safety (31). Fetal loss rates in the literature vary between 4% and 7% with preterm birth rates of 6% between 25 and 28 weeks' gestation and 22% before 33 weeks' gestation (32).
Fetal shunting procedures
In the early 1980s, several groups introduced the concept of ultrasound-guided fetal shunting procedures for a variety of conditions including fetal hydrocephalus, obstructive uropathy, and hydrothorax. Unfortunately, due to a lack of scientific evidence of therapeutic benefit these techniques have failed to become established fetal therapies.
Hydrocephalus
The improved neurological outcome following postnatal shunting of neonatal hydrocephalus generated significant enthusiasm for attempting prenatal therapy (33). Despite this initial enthusiasm, further studies failed to demonstrate an improvement in neurological outcome. The fetuses that underwent shunting procedures had in fact a poorer prognosis (34). This was thought to be secondary to underlying anomalies including migration disorders which could not be alleviated by shunting. Current clinical practice does not advocate the use of ventriculo-amniotic shunting for the management of fetal hydrocephalus.
Lower urinary tract obstruction
Lower urinary tract obstruction (LUTO) is a group of pathologies most commonly due to urethral atresia or posterior urethral valves which has an incidence of approximately 2.2 per 10,000 births (35). The clinical consequences of LUTO include renal dysplasia and dysfunction leading to oligohydramnios, pulmonary hypoplasia, and positional limb anomalies. Fetal LUTO without intervention is associated with a mortality rate of 45% (35). In those who survive, up to one-third develop end-stage renal impairment requiring dialysis or transplantation. Prenatal intervention was based on the belief that relieving the obstruction would potentially allow for normal lung development and prevent further renal damage. The technique of percutaneous vesicoamniotic shunting (VAS) involves the placement of a double pig-t ailed catheter under ultrasound guidance and local anaesthesia, with the distal end of the catheter in the fetal bladder and the proximal end in the amniotic cavity. Amnioinfusion prior to shunt insertion in cases of severe oligohydramnios may facilitate the procedure.
A meta-analysis of prenatal bladder drainage in LUTO demonstrated that despite improvement in survival, neonates who were treated prenatally had significant long-term morbidities (36). Subsequently, the Percutaneous Shunting in Lower Urinary Tract Obstruction (PLUTO) trial was conducted. This multicentre randomized controlled trial to investigate the role of fetal VAS in moderate or severe LUTO has reported short-term outcomes (37). Survival to 28 days and 1 year of life appeared to be higher with VAS than conservative management, but not conclusively so. The prognosis for both groups in terms of renal function was poor and VAS was substantially more expensive and unlikely to be regarded as cost-effective based on the 1-year data (37).
Hydrothorax
Fetal hydrothorax may present as an isolated accumulation of lymphatic fluid in cases of primary fetal hydrothorax or in association with non-immune hydrops secondary to structural anomalies. Primary fetal hydrothorax is a relatively uncommon condition with a prevalence up to 1 in 15,000 pregnancies (38). Although some hydrothoraces will resolve spontaneously, progression predisposes to pulmonary hypoplasia, hydrops, polyhydramnios, and preterm delivery. Approximately 57% of fetuses present with primary fetal hydrothorax complicated by hydrops with anticipated survival of 24% without treatment (39). As a consequence of significant associated morbidity and mortality, intrauterine therapy may be offered depending on gestational age, the size of the pleural collection, and secondary effects including the presence of hydrops. The aim of prenatal therapy is to remove the fluid from the chest in order to relieve intrathoracic pressure and its effects on pulmonary development and cardiovascular function. Therapeutic interventions to date have included thoracocentesis, thoracoamniotic shunting, and more recently pleurodesis. In a systematic review of278 cases of fetal hydrothorax managed with thoracoamniotic shunting, the reported overall survival was 63%, with a survival of 55% and 85% in hydropic and non- hydropic fetuses, respectively (40). The most common complications associated with the shunting procedure include PPROM, chorioamnionitis, and preterm delivery. Presently, there is no agreed consensus on the management of primary fetal hydrothorax. Most clinicians recommend that intervention should be reserved for hydropic fetuses, but a case may be made for those with large progressive effusions discovered at severe preterm gestations.