Historical background
‘Since antiquity various methods, many bizarre and some frankly dangerous, have been used in an attempt to bring on labour.’
Donald I (1955). Practical Obstetric Problems (1).
Informal methods for the induction of labour have been described for centuries. The use of ‘caster oil, hot bath and emema’ has been a common home technique and is thought to date back to Egyptian times. However, it was only in the eighteenth century that induction methods formally entered the medical literature (2). The first technique was amniotomy, described in 1756 by a London obstetrician, Thomas Denman and, as its popularity spread around Europe, it became known as the ‘English Method’. But in the absence of a uterotonic, amniotomy had little effect except in multiparous women. The understanding that the ease of induction as well as success rates related to the softness and dilatation of the cervix (not enumerated by Bishop in a formal score until 1964) led to attempts to prepare the cervix prior to amniotomy. This was commonly done forcibly using fingers or rubber bougies. In a detailed review of methods in 1861, Robert Barnes describes the wide variety of options for labour induction:
Some of these agents act directly upon the spinal marrow... such are ergot of rye, borax, cinnamon, and other drugs. Some evoke the energies of the diastolic system, by stimulating various peripheral nerves - such are rectal injections, the vaginal douche, the colpeurynter [an inflatable bag to distend the cervix], the carbonic-acid-gas douche, probably the irritation of breasts by sinapisms [a mustard plaster] and the air-pump, the cervical plug, whether in the form of sponge-tent or the caoutchouc [rubber] dilator, the separation of the membranes, the placing a flexible bougie in the uterus, the intrauterine injection, the evacuation of the liquor amnii, and galvanism [electrical muscle stimulation].
(3)He goes on to describe the technique of pushing a rubberized ‘fiddle-shaped’ bag through the cervix and then filling it with water so that it swelled both on either side of the cervix (3). This was to be repopularized 150 years later with the introduction of the cervical ripening balloon. A variant of this was the de Ribes’ bag, named after a Parisian accoucher, which was a reusable, rubber- covered, silk inflatable bag which was inserted through the cervix using special forceps and filled with water to a maximum of 500 mL (Figure 36.1).
The changes in medical advice about labour induction (Table 36.1) over the next 100 years were traced by Nabi et al. (2014) through the teaching in the 19 editions of the classic textbook Ten Teachers (4). Early in the twentieth century, methods were highly invasive, even brutal. As such, their use was restricted to cases of intrauterine fetal demise (IUFD) or severe maternal disease. In a mortality review of eight United Kingdom hospitals from 1925 to 1930, induction of labour was the direct cause of 5% of deaths in an overall maternal mortality rate of 424:100,000 (5). All cases were described as avoidable and were secondary to haemorrhage, sepsis, and anaesthetic complications.
Medical options with oxytocin and then prostaglandins started to become available in the twentieth century. The uterotonic effect of pituitary extract was described in 1909 by Sir Henry Dale, and first introduced into clinical practice by William Blair-Bell, an obstetrician from Liverpool who later founded the Royal College of Obstetrics and Gynaecology. But the major change came in the 1960s with the development of purified prostaglandins by Karim and colleagues in Makerere University, Uganda (6). Initially derived from semen, here was an agent that not only caused uterine contractions, but also simultaneously resulted in cervical ripening. Prostaglandin E2 is unstable and needs to be kept cold and given intravenously or vaginally.
The arrival of the stable prostaglandin Ei tablets (misoprostol) in the 1980s for gastric protection, allowed the same effect to be achieved by the oral, sublingual, or vaginal route.Induction rates have fluctuated widely with time and local culture. Despite the difficulties with induction, it became a very common practice in the medicalized days of the 1950s with up to 50% of all women undergoing induction in some hospitals. Rates fell after that, but have recently risen again. In the United Kingdom at the start of the twenty-first century, around 15% of all women were induced, but the rate has been steadily rising since then. Clinicians had been deterred by the association between labour induction and adverse outcomes. However, the recent finding that ‘induction without medical indication’ did not result in an increase in caesarean section or operative delivery and may even reduce adverse events has led to a steady rise in induction rates. In England today, the average induction rate is 30% with rates of over 40% in some hospitals.
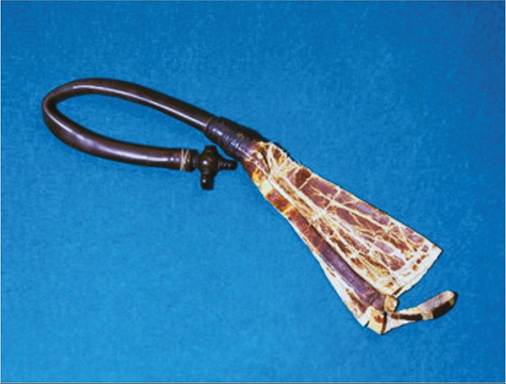
Figure 36.1 De Ribes' bag.