Instrumental vaginal delivery
A brief history of instrumental vaginal delivery
Instrumental vaginal delivery is performed using either forceps or a vacuum extractor, where traction force is applied on the fetal head to aid delivery in the second stage of labour.
The obstetric forceps were probably first invented at the end of the sixteenth century or during the early seventeenth century by the famous Chamberlen family of obstetricians, who took care of the royal family of England at that time. Designed for difficult childbirth, the prototype was kept secret by the Chamberlen family for more than 100 years. Since the mid eighteenth century, a variety of improvements in the design of forceps started to appear which made forceps delivery a popular solution for difficult childbirth. Subsequently, in 1849, Professor James Young Simpson designed the first vacuum extractor for childbirth with a simple design of a metal syringe attached to a soft rubber cup. However, the idea of using vacuum extraction to assist vaginal birth was not popular until the 1950s when Professor Malmstrom developed the ventouse with a metal cup connected to a vacuum pump machine. Vacuum extractors have now become a more favourable choice than forceps in many countries.Design of forceps
Obstetric forceps consist of two branches, and the basic structure of each branch includes the following (Figure 33.2):
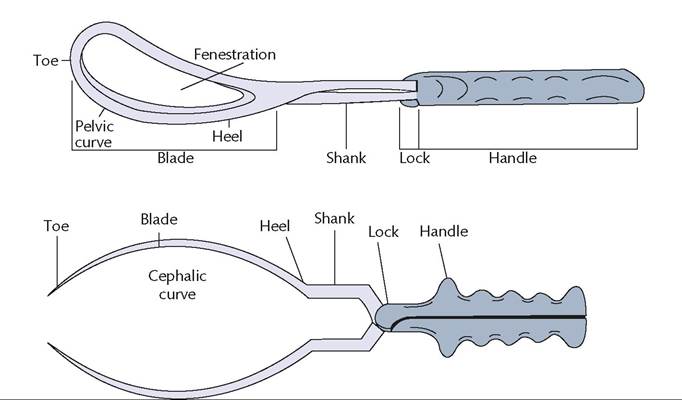
Figure 33.2 Figure showing the basic structure of forceps using Simpson's forceps as an example.
• The blade: this curved portion is to grasp the fetal head, with one blade on each side of the head. It characteristically has two curves, the cephalic and the pelvic curves, shaped to conform to the moulded and elongated fetal head and the birth canal respectively.
• The handle: allows pulling by the operators.
In Kielland’s forceps, it also allow rotation of malposition and sliding to correct asynclitism.• The shank: connects the blades and the handles. The axis of the blade is slightly tilted upwards from that of the shank in most of the forceps. However, the axis of the blade and the shanks are on the straight line in Kielland’s forceps to facilitate rotation. The shank is shorter in outlet forceps (Wrigely’s forceps) but longer in Kielland’s forceps. The shank of Piper’s forceps is long and bent downwards to facilitate delivery of the aftercoming head in vaginal breech delivery.
The lock is for keeping the two shanks together. Most forceps have a fixed lock design usually located at the junction of the shank and the handle. In rotational forceps (Kielland’s), it is a sliding lock design located along the shank.
There are different shapes of forceps which are designed for different purposes. Four characteristic forceps are shown in Figure 33.3 for comparison.
Design of vacuum extractor
The vacuum extractor consists of a vacuum cup which is designed in various sizes and diameters. The cup is attached or can be connected to a handle which allows the operator to apply traction force. The cup consists of a vacuum port which can be linked to the vacuum pump through a rubber tubing. There are several types as shown in the Figure 33.4 and described as follows:
• Bird cup (metal cup): this is a metal cup that is most commonly used. It is designed in various sizes of between 4 and 6 cm in diameter, and can be differentiated into an anterior or posterior cup. The posterior cup is specifically designed for use in the occipital posterior or lateral position or when the fetal head is deflexed.
• Silicon cup: the use of this type of soft silastic cup carries a higher incidence of failure than rigid vacuum cups because it is more likely to result in spontaneous detachment. However, they are less likely to be associated with scalp trauma. They are more suited for occipitoanterior (OA) positions.
• Kiwi OmniCup: this is a single-use, disposable, rigid plastic cup with an integral manual vacuum system incorporated into the hand-held device.
Indications of instrumental vaginal delivery
The incidence of instrumental vaginal delivery is approximately 510%, but varies widely between different countries. Instrumental vaginal delivery is indicated in the second stage of labour when vaginal birth is deemed possible but:
• the process has to be hastened because of fetal distress or maternal distress, or
• maternal pushing force needs augmentation because of maternal exhaustion, or
• prolonged second stage of labour
• maternal pushing force is not desirable because of maternal diseases such as cardiac diseases or neuromuscular diseases.
A prolonged second stage may be due to inadequate maternal pushing force or obstructed labour. The latter must be differentiated from the former by careful clinical examination, as it is an absolute contraindication of instrumental delivery. Wrong application of instrumental delivery in obstructed labour not only results in failure but also significant perinatal complications (e.g. birth asphyxia and cranial injury) and maternal complications (e.g. postpartum haemorrhage, perineal injury, and crash CS). Continuous support during labour, use of upright or lateral positions, and avoidance of epidural analgesia can reduce the need for operative vaginal delivery (6).
Classification of instrumental vaginal delivery
Depending on the station and position of the fetal head, instrumental delivery is classified into outlet, low-pelvic, and mid-pelvic levels as shown in Table 33.1. More difficulty is anticipated during the procedure when the level moves up. High-pelvic instrumental
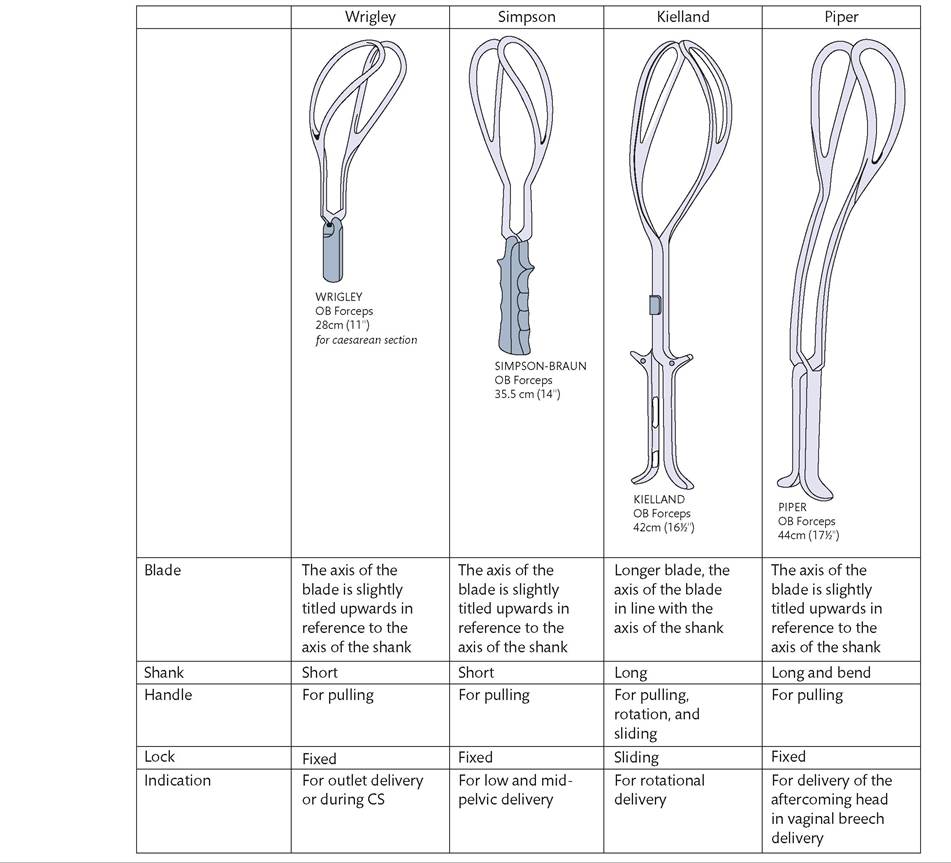
Figure 33.3 Comparison of different types of forceps.

Figure 33.4 The Bird cups, both anterior and posterior, silicon cup, and Kiwi OmniCup.

Table 33.1 Classification of instrumental vaginal delivery according to the station and position of the fetal head
| Level | Definition |
| Outlet | Fetal scalp is visible without separating the labia Fetal skull has reached the pelvic floor Sagittal suture is in the anteroposterior diameter or right or left occiput anterior or posterior position (rotation does not exceed 45 degrees) Fetal head is at or on the perineum |
| Low | Leading point of fetal skull (not caput) is at station +2 or more (lower) and not on the pelvic floor Two subdivisions: • Rotation of 45° or less from the occipitoanterior position • Rotation of more than 45° including the occipitoposterior position |
| Mid | Fetal head is no more than one-fifth palpable per abdomen Leading point of fetal skull is above station +2 but not above the ischial spines (i.e. below station 0) Two subdivisions: • Rotation of 45° or less from the occipitoanterior position • Rotation of more than 45° including the occipitoposterior position |
| (High) | NOT included in the classification as operative vaginal delivery is not recommended in this situation where the head is two- fifths or more palpable abdominally and the presenting part is above the level of the ischial spines |
Source data from American College of Obstetricians and Gynecologists. Operative vaginal delivery. ACOG Practice Bulletin No. 17. 2000.
delivery is nowadays regarded as a dangerous procedure and has been abandoned.
Prerequisites for instrumental vaginal delivery
The following prerequisites should be fulfilled to ensure a safe and successful instrumental vaginal delivery (8):
• The cervix must be fully dilated and membranes are ruptured.
• The fetal head should be well engaged and not more than one-fifth palpable per abdomen.
• The fetal head position and station must be known.
• The maternal pelvis is assessed to be adequate with no evidence of cephalopelvic disproportion (interspinous distance, subpubic arch, caput, and moulding in addition to station and position of the fetal head).
• The urinary bladder is emptied.
• There is adequate anaesthesia (forceps delivery should be performed under either regional anaesthesia or pudendal block while perineal local anaesthesia is acceptable for vacuum extraction).
• Procedure should be performed by a trained operator.
If vaginal delivery is not possible because of obstructed labour or cephalopelvic disproportion, a CS should be performed.
Choice of instrumental vaginal delivery
The preferences for forceps delivery and vacuum extractions vary between different countries. In the majority of indications, both instruments are applicable. However, forceps should be used instead of vacuum extraction in some less common situations such as gestation less than 34 weeks and face presentation where vacuum pressure may be dangerous to the fetus.
In case of vaginal breech delivery, only forceps can be applied for the aftercoming head, and Piper's forceps are the most suitable instrument for this purpose.In case the fetal head is not in the OA position, ordinary forceps are not applicable. In such situations, rotational forceps (using Kielland's forceps) delivery is more appropriate but it may increase maternal and perinatal morbidity. Hence, vacuum extraction may be a preferred choice to forceps in the non-OA position. This is because when the cup is properly applied over the vertex, it can then facilitate gradual autorotation of the fetal head to direct the OA position around the axis of the cup (over the vertex) as it descends the pelvic floor.
Procedure of forceps delivery
Application of forceps (use direct OA position as an example):
• Bladder is emptied.
• Adequate analgesia given either with pudendal block or regional anaesthesia.
• Check the forceps such that they can be paired and locked correctly.
• Apply lubrication onto the forceps blades.
• Using a pencil-grip to hold the shank of the forceps, the left blade is inserted into the maternal left side, followed by the right blade to the maternal right side.
• If the blades are applied correctly, they should be over the corresponding zygomatic regions of the fetus and the blades should lock easily.
• Check if both shanks are perpendicular to the maternal perineum and at the same length. If not, the forceps are not applied symmetrically and cannot be locked.
• After locking the forceps, check that the sagittal suture is cutting the shank perpendicularly, the space between the heel of the blade and the head allows only one finger (not one on one side and two on the other), and the occiput is 3-4 cm above the shank before traction is applied along the axis of the birth canal, that is, first downward and then upward (Figure 33.5).
• An episiotomy may be made when the fetal head crowns.
• Once the head is delivered, the forceps can be removed, and the rest of the body is delivered in the usual manner.
Risks and complications of forceps delivery
• Injury to the baby:
■ Laceration of the face and scalp, especially when the blades are applied incorrectly.
■ Facial nerve palsy.
■ Ocular trauma and retinal haemorrhage.
■ Skull fracture and/or intracranial haemorrhage: occasional but may result in brain injury.
• Injury to the mother:
■ Tears to the perineum and anal sphincters, extension to higher vagina or cervix, and pelvic floor injury.
■ Postpartum haemorrhage secondary to lower genital tract injury.

Figure 33.5 The direction of traction in forceps delivery.
Procedure of vacuum extraction
Application of vacuum cup:
• Bladder is emptied.
• Adequate local analgesia is given.
• Apply lubrication onto the vacuum cup.
• The cup is applied to the vertex in the midline over the sagittal suture, with the centre of the cup 3 cm in front of the posterior fontanelle, or 6 cm behind the anterior fontanelle. This is called the flexion point. Therefore, if a 6 cm cup is used, the rim of the cup is touching the posterior fontanelle, or 3 cm behind the anterior fontanelle. Correct placement of the cup at the flexion point (Figure 33.6) is crucial to promote flexion of the fetal head during delivery.
• After ensuring that maternal tissue is not trapped in the cup, the vacuum pressure is gradually built up to 60 cmHg in 2 minutes.
• Check again for any maternal tissues trapped between the fetal scalp and the cup.
• Once adequate vacuum pressure is achieved, a pulling force is applied coinciding with uterine contractions and maternal bearingdown effort along the axis of the birth canal (i.e. firstly downwards and then upwards).
• An episiotomy may be made when the fetal head crowns.
• Once the head is delivered, the vacuum cup can be removed, and the rest of the body is delivered in the usual manner.
Risks and complications of vacuum extraction
• Injury to the baby:
■ Subaponeurotic (subgaleal) haemorrhage: an uncommon but potentially life-threatening complication of vacuum extraction. Bleeding to the subaponeurotic space can be massive, but the diagnosis can be easily missed because of its insidious onset, and the masking effect of the coexisting caput or chignon created by the vacuum cup. It presents as a fluctuant boggy mass developing over the scalp, and in case of delayed diagnosis, the neonate presents with hypovolaemic shock.
■ Cephalohaematoma: unlike subaponeurotic haemorrhage, cephalohaematoma is subperiosteal bleeding which is bounded by sutures, and hence is usually self-limiting.
■ Intracranial haemorrhage and skull fracture: occasionally happens in difficult vacuum extraction but can result in severe brain injury.
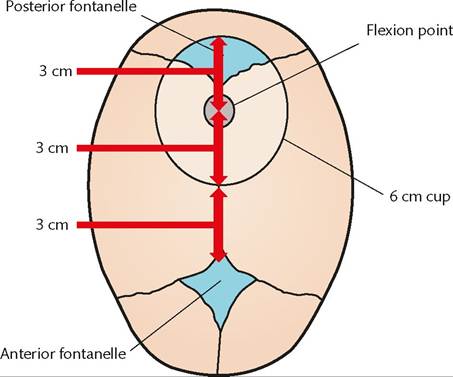
Figure 33.6 The correct position of the cup at the flexion point.
• Injury to the mother:
■ Perineal and pelvic floor injury (less common than forceps delivery).
■ Cervical or vaginal tears if the tissues are accidentally trapped by the vacuum pressure into the cup.
■ Postpartum haemorrhage secondary to lower genital tract injury.