Caesarean section
A brief history of caesarean section
While the exact origin of the name ‘caesarean’ remains unclear, it is often wrongly attributed to the birth of Julius Caesar, who was mistakenly thought to have been born after his dying mother’s abdomen was cut open.
Operative abdominal birth was mentioned in legends of various ancient civilizations before Caesar’s era, such as the birth of Jilian, the founder of the State of Chu in China 3000 years ago, and that of Bindusara, the second emperor of the Maurya Empire in India in the third century âńĺ, but perhaps the first well-recorded case of CS with maternal survival was performed in the sixteenth century, by a pig gilder called Jakob Nufer on his wife who suffered from prolonged labour. The maternal mortality of CS remained very high (85% in the nineteenth century in Great Britain) until the introduction of the lower segment uterine incision technique and other surgical improvements since the beginning of the twentieth century.Indications for a caesarean section
CS is indicated when vaginal delivery is not likely to be successful, or poses substantial risk to the mother or to the fetus. If the fetus (the passenger) is relatively too big to pass through the birth canal (the passage), or when the uterine contraction (power) is insufficient or uncoordinated, vaginal delivery would become unsuccessful, such as in the following conditions:
• Contracted maternal pelvis or cephalopelvic disproportion
• Macrosomia (risk of shoulder dystocia)
• Abnormal fetal lie causing malpresentation (e.g. transverse lie)
• Fibroids in the lower segment causing non-engagement of fetal head
• Poor progress of labour (may be due to obstruction or poor contractions)
• Failed induction of labour
• Failed instrumental delivery
• Congenital malformations with high risk of obstructed labour
(e.g.
hydrocephalus).Conditions where vaginal delivery may increase the maternal risks include:
• placenta praevia (causes significant antepartum haemorrhage as well as non-engagement of the fetal head)
• maternal complications (e.g. eclampsia)
• maternal cardiac diseases.
Conditions where vaginal delivery may increase the fetal risks include:
• a severely growth-restricted fetus who cannot sustain the stress of labour
• placental abruption, cord prolapse, intrauterine infection, and other causes of fetal distress which require immediate delivery (some of these conditions also impose maternal risk)
• previous classical CS or previous myomectomy (in particular with an incision entering into the uterine cavity) of which the scars are at risk of rupture during labour, and hence fetal distress (the mother is also at risk of haemorrhage in such a situation)
• vasa praevia where vaginal delivery is associated with a high risk of fetal haemorrhage due to the rupture of the placental vessel
• active genital herpes infection or maternal HIV, in which case avoiding vaginal delivery by planned elective CS may reduce the transmission of the disease to the fetus during labour.
The incidences of CS vary significantly from country to country, with a wide range of below 10% to higher than 50% (1). The very high CS rates in many countries are not because of medical indications but social reasons, such as maternal anxiety towards labour pain and concerns about fetal risk during labour. Although CS is a very safe surgical procedure, it may impose risks on the mothers in their subsequent pregnancy, as well as long-term negative implications for health resources. An unnecessary CS without a medical indication should be avoided.
Types of caesarean incision
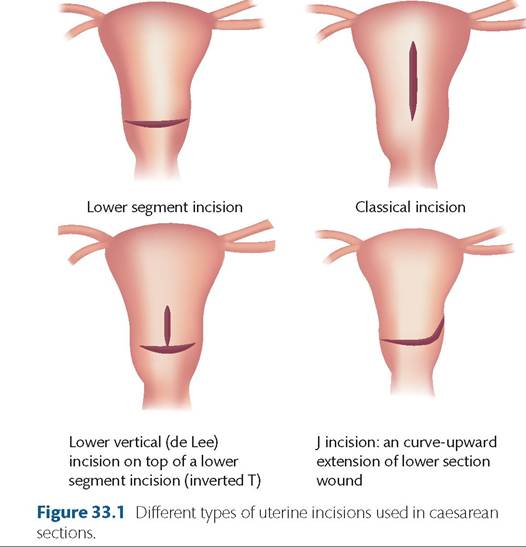
Lower segment incision
This is the most common type of caesarean incision performed nowadays (Figure 33.1). This involves a transverse incision (Kerr incision) of the lower segment of the uterus, which is developed from the expansion of the isthmic region of the uterus.
The risk of rupture of scar at this non-contractile portion of the uterus in the subsequent pregnancy is significantly lower than that of a classical incision (0.20.5% vs 4.0-9.0%). Furthermore, it is associated with less blood loss and easier uterine closure because of the thinner muscle wall at the lower segment.Classical incision
Historically, CS was performed with a vertical incision at the anterior fundus of the uterus. Due to the significantly increased risk of scar rupture and higher complication rate, the classical incision (Figure 33.1) has been replaced by lower segment incision, and is nowadays restricted to conditions where access to the lower segment is deemed not possible or with considerable risks, or when the lower segment is not well developed. As the lower segment only begins to form at around 28 weeks' gestation, CS prior to this gestation time may necessitate a classical incision. The indications for classical CS are listed in Box 33.1.
Lower vertical (de Lee) incision
This is a vertical incision at the non-contractile lower segment, but it may extend to the upper part of the uterus (Figure 33.1). It is seldom
Box 33.1 Common indications of classical caesarean section in modern obstetrics
• Preterm caesarean delivery where lower segment is not well formed (especially before 28 weeks).
• Lower segment fibroid or cervical fibroid.
• Placenta praevia with large vessels at lower segment.
• Placenta accreta involving the lower segment.
• Fetal malformation where the lower segment would not allow sufficient room for infant to be delivered (e.g. conjoined twins).
• Fetal transverse lie (in particular with fetal back down) may need a classical incision.
• Perimortem CS (swift delivery is required).
performed but may be required when the transverse incision of the lower segment does not allow enough room for delivery of the fetus (e.g.
transverse lie). The combination of a lower vertical and lower segment incisions form an inverted T incision.J incision
This is a curve-upward extension from one end of a lower segment incision during a difficult delivery, so as to avoid tearing of the uterus laterally to the board ligament (Figure 33.1).
Procedure and operative technique
Preoperative preparation
Women are kept fasting before the operation. The risks of the operation must be discussed thoroughly with consent signed. Antacids are given routinely as premedication to reduce the risk of aspiration pneumonitis. Although the chance of transfusion is not high in uncomplicated CSs, a preoperative haemoglobin level should be checked and the type and screen should be saved. Where there is a high risk of bleeding, for example, placenta praevia, blood products must be readily available. A pneumatic cuff or pressure stockings are worn to reduce the risk of deep vein thrombosis. Preoperative ultrasonography may be helpful in certain circumstances, such as mapping the placenta in cases of placenta praevia or accreta. Women are kept in the left lateral tilt position on the operating table to prevent aortocaval compression which could lead to maternal hypotension and uteroplacental insufficiency. A Foley catheter is inserted following anaesthesia to empty the bladder. Prophylactic antibiotics, preferably cephalosporins, are given on induction to prevent wound infection.
Anaesthesia
Regional anaesthesia (either spinal, epidural, or combined spinal- epidural anaesthesia) is the most common and a safer method of anaesthesia compared to general anaesthesia. It allows earlier mobilization and is preferred by most women as they remain awake and can experience the birth of their child. Epidural anaesthesia can also be used for postoperative pain relief. Volume preloading and administration of ephedrine or phenylephrine can reduce the risk of hypotension associated with regional anaesthesia. With general anaesthesia, there are risks of maternal aspiration pneumonitis and difficulty in intubation because of the oedema related to pregnancy (or pregnancy-related complications such as pre-eclampsia).
In addition, the anaesthetic agents may cause depression of the infant immediately after birth. Therefore, general anaesthesia is only limited to certain cases where regional anaesthesia is contraindicated, or an extremely difficult CS is anticipated.Abdominal incision
Aseptic reagents (e.g. povidone iodine or chlorhexidine gluconate) are used for skin preparation. The choice of skin incision depends on the gestation, the presence of previous scar, and the need of classical CS. CS is mostly performed through a transverse incision, either through a Pfannenstiel incision or Joel-Cohen incision. The Joel-Cohen incision is made by blunt dissection by fingers in deeper layers of the abdominal wound, which may be more difficult where scar tissues are present in cases of repeat CSs. Transverse incisions are preferable because they reduce wound pain, wound breakdown, incisional hernia, and have a better cosmetic result.
Where classical CS is planned, a subumbilical midline vertical incision should be made to facilitate a longitudinal incision of the uterus. Very occasionally, a paramedian incision is made which allows extension above the umbilicus when necessary.
Uterine incision and wound repair
Lower segment wound
Dissection of the bladder with the bladder flap pushed inferiorly is necessary to allow exposure ofthe lower segment ofthe uterus. The uterine incision should not be made too low to avoid injuring the cervix. This is especially true following prolonged labour, CS at the second stage, or after failed instrumental delivery, where the cervix may be drawn upwards. Occasionally, extension of a lower segment incision may be necessary to allow more room for delivery of the infant, either through a J incision or inverted T incision (Figure 33.1). With these types of complicated incisions, the risk of scar rupture in future pregnancies may increase. After the delivery of the fetus and the placenta (see later), the lower segment incision is usually closed in two layers.
Classical wound
A vertical incision is made on the anterior uterine wall at the upper part of the uterus (Figure 33.1), and hence dissection of the bladder is not necessary. However, this upper part of the uterus has a thick myometrial wall which would lead to more blood loss when compared to a lower segment incision. The classical uterine incision is closed in three layers.
Delivery of the fetus
Cephalic presentation
The posterior aspect of the fetal head is cupped and elevated from the uterine cavity. Fundal pressure can be applied to aid delivery of the fetal head out through the uterine wound. Disimpaction of the fetal head may be necessary if it is engaged into the maternal pelvis, especially in cases of prolonged labour, second-stage CS, or caesarean delivery following failed instrumental delivery. An inferior or lateral uterine tear of the lower segment may result if this step is not performed smoothly. An inferior tear could extend to the cervix or vagina making repair difficult, and a lateral tear could lead to heavy bleeding from the uterine vessels or haematoma formation in the broad ligament. It is crucial that repair is performed properly with haemostasis well secured. In cases where the fetal head is high and has failed to be delivered by fundal pressure, the use of forceps can aid the delivery of the fetal head. Following the delivery of the head, the shoulders and rest of the body can be delivered smoothly.
Breech presentation
In the event of an extended breech, the fetal buttocks are firstly elevated and delivered from the uterine wound. Alternatively, the baby's buttocks can be lifted out from the uterine wound by hooking them bilaterally by the operator. If the baby is in footling breech, the fetal feet are grasped and delivered from the uterine wound. The rest of the baby is delivered by breech extraction, where the arms are delivered by the Lovset manoeuvre, and the fetal head by the Mariceau-Smellie-Viet manoeuvre, in a similar manner as in vaginal breech delivery (as described in the last section of this chapter).
Transverse or other abnormal fetal lie
Ultrasonography prior to the operation may be performed to locate the fetal spine and feet. During the delivery, the fetal lie should first be converted into longitudinal, usually by grasping the fetal feet followed by traction which will then bring the buttocks to the lower segment. The fetus can then be delivered as in breech presentation. Failure to convert into longitudinal lie may occur when the upper limb(s) is/are wrongly grasped and pulled, or when the amniotic membrane is ruptured prematurely, resulting in reduction of amniotic fluid and shrinking of the uterine cavity, which in turn restrict further turning of the fetus. If this happens, extension of the uterine wound or an additional vertical incision may be needed to deliver the transversely lying fetus. Any delay in delivery at this stage may cause fetal hypoxia and birth asphyxia.
Delivery of the placenta
Syntocinon 5 IU is routinely administered intravenously after delivery of the baby to encourage uterine contraction and to reduce blood loss. The placenta may be expelled spontaneously. If not, the placenta can be delivered by applying fundal pressure or controlled cord traction. Only if these measures fail, the placenta can be removed manually by separating it from the uterus by the operator's hand; however, this is associated with an increased risk of blood loss and endometritis. The uterine cavity should always be checked and emptied with complete removal of the placenta.
Closure of the abdominal wall
Closure of the peritoneum is not necessary. The rectus sheath is closed with continuous absorbable sutures. Routine closure of the subcutaneous layer is not necessary, unless the woman has more than 2 cm subcutaneous fat. Skin can be closed by subcuticular continuous sutures. Interrupted mattress sutures are preferred in obese patients.
Postoperative care
Adequate analgesia should be given following CS. Women should be encouraged to have adequate hydration, early mobilization, and graduated stockings to reduce the risk of venous thromboembolism. High-risk women should be given low-molecular-weight heparin. Haemoglobin should be checked if there is significant blood loss. Discussion with the woman about future childbearing and mode of delivery should be provided.
Risks and complications of caesarean section
Short term
Maternal
• Haemorrhage mainly from the uterine wound, occasionally from the wound of the abdominal wall. Small risk of hysterectomy in cases of massive haemorrhage.
• Uterine injury (e.g. uterine tear).
• Wound infection.
• Endometritis.
• Visceral injury, most commonly the bladder.
• Urinary tract infection (after urinary bladder catheterization).
• Venous thromboembolism.
• Complications related to regional or general anaesthesia.
Fetal injury
• Fetal skin lacerations due to an untended cut made during the incision of the uterine wall.
• Fetal musculoskeletal or cranial injury during obstructed delivery through the uterine wound.
• Fetal birth asphyxia due to delayed/obstructed delivery through the uterine wound.
Long-term implications in future pregnancies
• Risk of scar rupture in future pregnancy:
■ Lower transverse scar: 0.2-0.5% (2).
■ Classical scar: 4-9% (3).
• Risk of placenta praevia and placenta accreta in subsequent pregnancy.
• Risk of ectopic scar pregnancy.
Vaginal birth after caesarean section
Vaginal birth after caesarean section (VBAC) can be offered to women with history of a single uncomplicated lower segment CS, and where there are no contraindications for vaginal birth in the current pregnancy. The benefits of a VBAC are the avoidance of the associated anaesthetic and surgical risks involved in a CS, faster recovery, and shorter hospital stay. More importantly, it reduces the risk of placenta praevia or placenta accreta in future pregnancies, as this complication is associated with repeated CSs.
The successful rate of a VBAC is approximately 75% (4). A previous vaginal delivery increases the success rate. With a history of successful VBAC, the success rate increases up to 90%. Contraindications of VBAC include the following:
Absolute contraindications:
• Classical caesarean scar (high risk of scar rupture).
• History of uterine rupture.
• Presence of contraindications for vaginal birth (e.g. placenta praevia).
Relative contraindications:
• Complicated uterine scars.
• Two or more previous lower segment CSs.
• History of myomectomy (especially in the myomectomy incision has entered the uterine cavity).
Complications of VBAC:
• Risk of emergency CS during VBAC.
• Scar rupture (0.2-0.5% following one uncomplicated lower segment CS).
• Fetal asphyxia, perinatal death, and maternal haemorrhage in the event of scar rupture.
Management of labour in women undergoing VBAC (5):
• Delivery should be in a hospital setting where immediate caesarean delivery and advanced neonatal resuscitation facilities are readily available.
• There is a two- to threefold increase in risk of uterine rupture if labour is induced or augmented. If induction of labour is necessary, a mechanical method of induction (e.g. amniotomy, balloon catheter) may be preferred to reduce the risk of scar rupture associated with the use of oxytocin or prostaglandins.
• Continuous cardiotocography (CTG) should be provided.
• Progress of labour should be monitored for evidence of obstructed labour where emergency CS would be necessary.
• Symptoms and signs of scar rupture should be closely monitored. These include:
■ abnormal CTG
■ severe abdominal pain persistent in between contractions
■ scar pain and tenderness
■ vaginal bleeding
■ haematuria
■ evidence of shock of the mother
■ loss of presenting part, change in abdominal contour, fetal parts are easily felt per abdomen.
More on the topic Caesarean section:
- REFERENCES
- References
- Psychological/social aspects of prolonged pregnancy
- Anticipating problems
- The INTERGROWTH-21st Project
- REFERENCES
- REFERENCES
- Managing the obstetric aspects of stillbirth
- REFERENCES
- Pregnancy management