Introduction
The word ‘placenta’ comes from the Latin term for ‘cake’. Historians and cultural anthropologists have explored cross- cultural beliefs and practices that invest the afterbirth with symbolic value, whether it is buried, burned, frozen, or eaten (1).
The first known representation of a human placenta can be found on the Narmer Palette (Figure 9.1). Narmer was an Egyptian pharaoh of the Early Dynastic Period (31st century âń) and the ancient Egyptians believed the placenta to be the ‘seat of the human soul’. The placenta was mummified immediately after the birth of the future pharaoh, used in dynastic processions, and buried in the tomb at the time of the pharaoh’s death.The development of a placenta is characteristic of those mammalian species called the ‘placentals’. True placentals probably originated after the significant extinction horizon known as the Cretaceous-Paleogene event 66-65 million years ago (2). The majority of mammals are placentals, meaning that their fetus (or fetuses) is nourished by the placenta during the entire pregnancy and develops entirely inside the placental membranes. In most mammals, the yolk sac and chorion combine to form a choriovitelline placenta to support the early embryo, although a chorioallantoic placenta soon supplants this. Humans and haplorrhine primates follow a second pattern where precocious development of the extraembryonic mesoderm leads to formation of a secondary yolk sac within the exocoelom (3).
Scientific investigations of the development, structure, and function of the placenta can be traced to antiquity (4). An issue of importance that was only resolved in the late eighteenth century is that of the separate nature of the maternal and fetal placental circulations. The breakthrough came in 1754, when John Hunter (1728-1793), who is considered the father of modern surgery, injected coloured molten wax into the vessels of the umbilical cord and the uterine arteries and veins during autopsies of pregnant women (4).
Assisted by Colin MacKenzie (died 1775), he demonstrated conclusively that the maternal and fetal circulations are separated, thus putting to rest a debate that had gripped anatomists for many centuries, including Galen (130-210), Leonardo Da Vinci (1452-1519), and Vesalius (1514-1564).Twentieth-century researchers have established that the placenta in mammals is the essential interface between the maternal circulation carrying oxygen-rich blood and nutrients, and the fetal circulation. No organ can match the placenta for the diversity of its functions, since it performs the actions of all the major organ systems while these differentiate and mature in the fetus (5). During the course of a pregnancy, it acts as the lungs, gut, kidneys, and liver of the fetus. The placenta also has major endocrine actions that modulate maternal physiology and metabolism.
From the perspective of laypeople, the twentieth-century perception of the placental barrier that is most readily available is a simple one: ‘we’ once thought that the fetus was protected from external insult by the placenta (1). Recent changes in human environmental habitats caused by pollution, habits such as smoking, and the increased use of medical and recreational drugs have challenged the concept of a complete protective role of the placental barrier. The thalidomide and diethylstilbestrol teratogenic catastrophes tragically illustrate its limitations (1, 5). By contrast, recent data from metagenomic sequencing show that the placenta is frequently colonized with maternal commensal bacteria during pregnancy, and indicate the selective role of the placental barrier and indirectly its additional metabolic and immune contributions to the developing fetus (6).
Aberrations of placental function are widely recognized as having immediate consequences on the outcome of a pregnancy, and more recently for influencing the lifelong health of the offspring. It is notable, for example, that the placenta grows more slowly during the first trimester in pregnancies that subsequently go on to miscarry or are associated with fetal growth restriction (FGR) than in normal cases (7).
Recent changes in human lifestyle, such as delayed childbirth and hypercaloric diets, may have increased the global incidence of placental-related disorders over the last decades. However, the fact that populations of hunter-gatherers still in existence today are affected by these pregnancy complications suggests that they are not a direct consequence of the modern human lifestyle, but are more likely to be due to an evolutionary step in human reproduction and development (8).This chapter presents an overview of the normal and abnormal development of the human placenta, together with a description of the physiology of placental biological functions, an analysis of the pathophysiology of placental-related disorders, and the prenatal diagnosis and management of placental and cord anomalies.
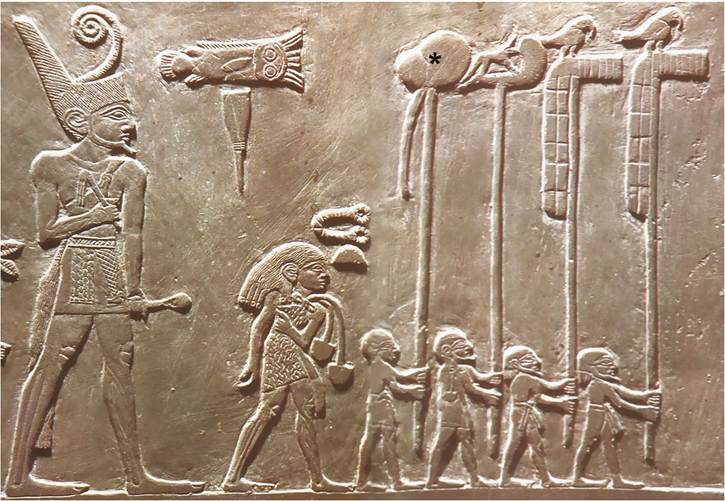
Figure 9.1 Photograph of the Narmer Palette (Early Dynastic Period; Egypt 31st century bc) showing the dynastic procession of the pharaoh Narmer preceded by a priest and four attendants, the first one carrying the placenta (star).