Malposition
The malpositions associated with a vertex presentation include occipitoposterior (OP) or occipitotransverse (OT) and arrested progress may result from a persistent OP position or deep transverse arrest.
The chin (mento) is the denominator for a face presentation and a mentoanterior position is suitable for spontaneous vaginal delivery. Persistent mentotransverse or mentoposterior positions are likely to result in obstructed labour and delivery by caesarean section. For breech presentation, the fetus can deliver vaginally in the optimal sacroanterior position but is considered a malposition if orientated in a sacroposterior position, as the fetal head will be orientated in an OP position following delivery of the body.If the fetus has engaged in an OP position, internal rotation can occur from an OP to an OA position. This long internal rotation may explain the increased duration of labour associated with OP position. Alternatively, an OP position may persist, resulting in a ‘face to pubes' spontaneous delivery. However, the persistent OP position may be associated with deflexion of the fetal head and a resulting increase in the diameter presenting to the pelvic outlet (Figure 32.1). This may lead to obstructed labour and the need for instrumental delivery or caesarean section. A deep transverse arrest may occur as a result of a head that has engaged in the transverse position and fails to rotate to OA or a head that engages in an OP position and only partially rotates to OT.
Aetiology
The aetiologies of vertex malposition (OP and OT) are represented by each of the 3 Ps. The fetal head may fail to rotate due to inefficient uterine activity in the first or second stage of labour or insufficient maternal expulsive efforts in the active second stage. This may be precipitated or aggravated by supine positioning of the mother and/ or use of epidural analgesia.
A Cochrane systematic review reports an average 14-minute increase in the duration of the second stage of labour and 1.4-fold increase in the incidence of operative vaginal delivery (OVD) with use of epidural analgesia in labour (odds ratio (OR) 1.42; 95% confidence interval (CI) 1.28-1.57) (12).The shape and dimensions of the maternal pelvis have an important contributory role in fetal malposition. The gynaecoid pelvis with a round shape, well-curved sacrum, and subpubic arch of approximately 90 degrees is the preferred shape for labour and an android-, anthropoid-, or platypelloid-shaped pelvis may lead to failure of engagement, descent, or rotation (Figure 32.5). Epidural analgesia is thought to relax the pelvic floor musculature and reduce the maternal urge to push which may lead to incomplete flexion and rotation of the presenting part. The extremes of fetal size may contribute to fetal malposition; a very large fetus with relative disproportion may rotate with difficulty and a small fetus may engage with a deflexed attitude or with marked asynclitism that limits spontaneous rotation.
Diagnosis
Vaginal examination during the course of labour allows a systematic assessment of the fontanelles and sutures of the fetal head. The anterior fontanelle is larger, softer, and has four radiating sutures in comparison to the posterior fontanelle which is smaller, firmer, and has three radiating sutures. It should be possible to diagnose OT and OP positions and to define the orientation in terms of direct, right, or left. Examination is more difficult in the context of marked caput, moulding, a high presenting part, maternal obesity, or poor analgesia. Asynclitism results in an oblique orientation of the presenting part and is often associated with malposition. This can complicate assessment, as the sagittal suture will be deviated from the midline to the right or the left for OA-OP positions and deviated superiorly or inferiorly for left OT-right OT positions (13).
The partogram may provide important clues to suggest a malposition. As with malpresentation, there may be primary arrest or slow progress despite good contractions in nulliparous labour. A secondary arrest or arrest in the second stage of labour should raise suspicion of a malposition in both nulliparous and multiparous women (Figure 32.2).
The role of ultrasonography in labour has developed in recent years and it is particularly useful when there is clinical uncertainty about the fetal head position (14) (Table 32.1). A multicentre randomized controlled trial (RCT) reported a 20% error rate in the clinical diagnosis of the fetal head position immediately prior to instrumental delivery that was reduced to 1.6% with the use of ultrasonography (15) (Figure 32.6). Three-dimensional ultrasonography has been used to measure the subpubic arch demonstrating an association between a narrow arch and a higher risk of persistent posterior occiput position at birth (16). The ultimate confirmation of the fetal head position is at the time of birth and this should be documented at emergency caesarean section to help explain the need for operative delivery.
Prevention
Although it is logical to promote maternal positions that widen the pelvic diameters and increase gravitational forces, there is little evidence that manoeuvres such as ‘all fours' used prophylactically reduce the incidence of OP or OT positions at delivery (17). However, a systematic review that assessed the benefits and risks of the use of different positions during the second stage of labour reported a reduced duration of the second stage: a weighted mean reduction in duration of 16.9 minutes (95% CI 14.3-19.5 minutes) and a reduction in assisted births (relative risk (RR) 0.84; 95% CI 0.73-0.98) (18).
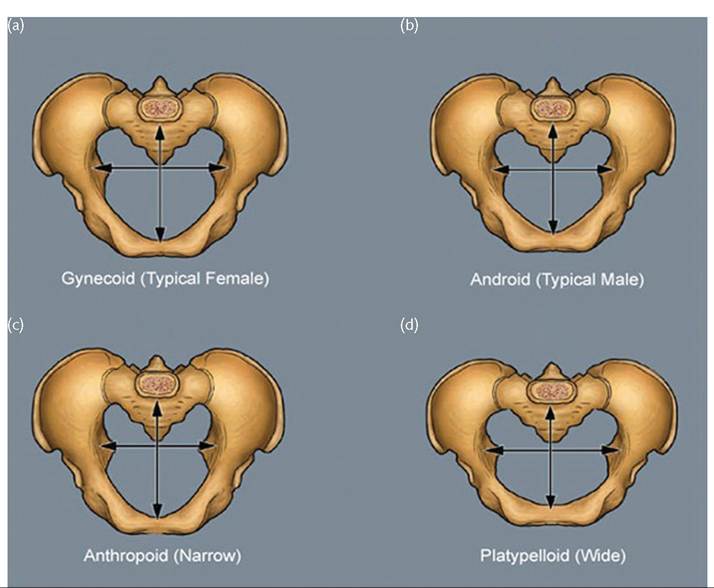
Figure 32.5 Pelvic shapes. (a) Gynaecoid pelvis—'round female shape' favourable for vaginal delivery (50% women).
Inlet transverse diameter greater than AP shallow cavity, short ischial spines, and wide subpubic arch. (b) Anthropoid pelvis—'long oval shape' vaginal delivery possible, favours OP (25% white/40% black women), AP greater than transverse, long narrow canal and sacrum, and wide subpubic arch. (c) Android pelvis—'male heart shape' unfavourable for vaginal delivery (20% women). Narrow inlet, prominent ischial spines, and narrow transverse outlet and subpubic arch. (d) Platypelloid pelvis—'kidney shape' 'unfavourable for vaginal delivery (5% women). Pelvic inlet transverse diameter much greater than AP sacral promontory pushed forward.Avoiding epidural analgesia will eliminate the epidural- associated risks of malrotation; however, for women who choose regional analgesia, a passive phase of at least 1 hour should be encouraged to facilitate descent and rotation of the fetal head (19-22). Judicious use of oxytocin should be considered where contractions dissipate; however, an RCT evaluating routine use of oxytocin during the second stage of labour in nulliparous women using epidural analgesia demonstrated a reduction in the operative delivery rate but only when the occiput was anterior (23).
Manual rotation has been explored as a strategy to correct fetal malpositions and is recommended in the guideline of the Society of Obstetricians and Gynaecologists of Canada (24). A large, retrospective cohort study reported a reduction in caesarean delivery associated with the use of manual rotation (9% vs 41%; P for a Cochrane systematic review comparing OVD with caesarean section for difficult deliveries in the second stage of labour, as yet there have been no RCTs addressing this important question. In current practice, the decision relies on observational data, national guidelines, experience, judgement, and clinical skill (21, 22, 24, 26).
In a United Kingdom-based prospective cohort study of women transferred to theatre for second-stage arrest, two-thirds of whom had a malposition, it was possible to achieve delivery by vacuum or forceps in half the cases (27).
The success rate was significantly higher among experienced operators. Caesarean section was associated with an increased risk of major haemorrhage (adjusted odds ratio (aOR) 2.8; 95% CI 1.1-7.6) and prolonged hospital stay (aOR 3.5; 95% CI 1.6-7.6). High rates of obstetric anal sphincter injury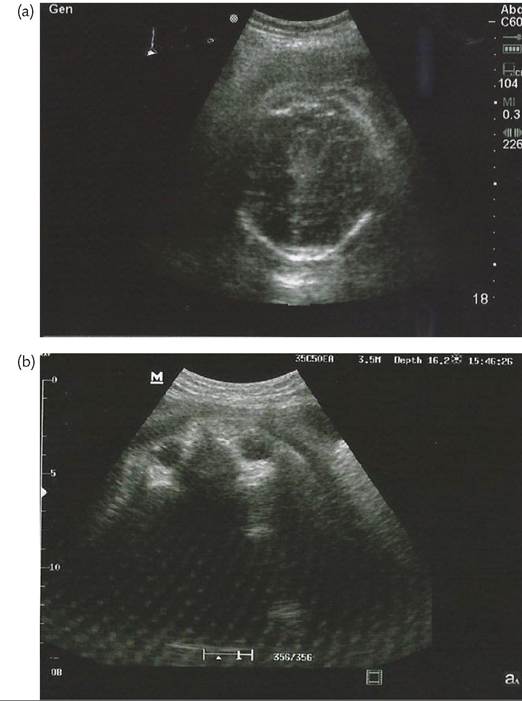
Figure 32.6 Fetal orbits and nose indicating an Occipitoposterior position. This image has been taken on a portable ultrasound machine on the labour ward during labour.
Manual rotation versus rotational vacuum versus
rotational forceps
Malposition in the second stage of labour requires both rotation and traction if vaginal delivery is to be achieved. These processes occur simultaneously with rotational vacuum delivery and are consecutive with rotational forceps and manual rotation followed by direct traction forceps. Some operators will choose to deliver an OP position with direct traction forceps ‘face to pubes'; however, given the wider presenting diameter, this is a more traumatic delivery with a higher incidence of OASI and should only be contemplated when the vertex is very low in the pelvis. The choice between forceps or vacuum delivery will depend on the operator's competence and preference for the clinical circumstances (32) (Box 32.1). As with any OVD, safety criteria have to be met and clear stopping rules should be observed (21, 22).
Successive systematic reviews of RCTs comparing vacuum and forceps report that use of the vacuum extractor is associated with significantly less maternal trauma (OR 0.41; 95% CI 0.33-0.50) (33). However, vacuum failure rates of between 20% and 30% have been reported in two RCTs comparing different vacuum devices, and failure of vacuum delivery was three to four times more likely with a fetal malposition (34, 35). Two United Kingdom-based observational studies compared rotational vacuum, manual rotation with traction forceps, and Kielland's rotational forceps, and reported similar maternal and neonatal morbidity rates but a higher failure rate with attempted rotational vacuum delivery (36, 37).
A furtherBox 32.1 Mid-pelvic rotational delivery
(8%) were reported following OVD and there was a threefold increased risk of urinary incontinence at 3 years compared to second- stage caesarean section (28). The comparable morbidity at caesarean section related to extension of the uterine incision into the cervix, vagina, or broad ligaments (24%) and a far higher repeat caesarean section rate in subsequent pregnancies (79% vs 31%) (29).
There is inconsistency in the reported early neonatal morbidity when comparing OVD with caesarean section in the second stage of labour. In the prospective cohort study described earlier, delivery by caesarean section was associated with an increased risk of admission to the special care baby unit (aOR 2.6; 95% CI 1.2-6.0); however, neonatal trauma was significantly less common (aOR 0.4; 95% CI 0.2-0.7) (27). Reassuringly, a 5-year follow-up of the cohort reported low overall rates of neurodevelopmental morbidity with comparable outcomes for each mode of delivery (30). These findings suggest that neonatal complications can be minimized with careful selection of cases for attempted OVD.
Fetal malposition is highlighted in many studies as a risk factor for failed OVD and as such, precautions should be taken to provide immediate access to emergency caesarean section should it be required. The additional time taken to transfer a woman to an operating theatre needs to be balanced with the consequences of a failed attempt at OVD in a delivery room (31). This issue is addressed in Having judged that attempting OVD is suitable, the following factors influence the selection of a particular method.
• Select manual rotation and traction forceps if:
— good analgesia
— rotational movement is possible
— descent of fetal head with maternal effort
— birth canal is roomy
— absence of signs of true CPD.
• Select Kielland's forceps if:
— dense regional block
— descent of fetal head with maternal effort
— birth canal is roomy
— absence of signs of true CPD.
• Select vacuum (with metal cup or Kiwi OmniCup) if:
— no dense regional block
— good maternal effort
— descent of fetal head with maternal effort
— no significant caput/moulding
— no signs of true CPD.
• A method should only be used if the operator is adequately trained.
• The operator should use the instrument he or she prefers.
• Mother's preferences should be taken account of where appropriate.
• Vacuum contraindicated at gestational age marked caput and moulding. Labour is likely to arrest in the first stage, but when full dilatation is reached, these findings preclude any attempt at OVD and delivery will be by caesarean section. The difficulty arises with the correct diagnosis of relative CPD which should be considered with the following features:
• Fetal head is slow to engage.
• Fetus palpates large relative to the maternal size.
• Progress is slow or arrests despite efficient uterine contractions.
• Vaginal examination shows early moulding and caput formation.
• Head is poorly applied to the cervix.
• Progressive oedema of the cervix.
• Haematuria.
As with malpresentation and malposition, the partogram may give clues to the presence of CPD. There may be primary arrest or slow progress despite good contractions in nulliparous labour, and secondary arrest or arrest in the second stage of labour should raise suspicion of potential CPD in both nulliparous and multiparous women (Figure 32.2).
Prevention
X-ray pelvimetry has been used in the past to determine the various dimensions of the pelvic inlet, mid pelvis, and outlet, primarily to inform the delivery method for breech presentation or birth after caesarean section. This practice was largely discontinued due to the poor predictive value of pelvimetry for successful vaginal delivery (40). Magnetic resonance imaging and three-dimensional ultrasonography have been evaluated in observational studies but have not been implemented at a population-based level to determine which women are likely to encounter obstructed labour as a result of CPD. Prevention is currently based on case selection with an individualized approach to offering caesarean section, for example, to women who have diabetes in pregnancy complicated by fetal macrosomia. A recent multicentre RCT reported that induction of labour from 38 weeks’ gestation compared to expectant management for women with large-for-gestational age fetuses (abdominal circumference >95th percentile) resulted in less traumatic injuries without an increase in delivery by caesarean section (41). It now seems appropriate to offer selected women with large fetuses an induction of labour at term in the interests of avoiding additional fetal weight gain and the potential for CPD.
Management
The principles for managing suspected CPD are similar to that of malposition. In the first stage of labour when progress arrests due to suspected CPD, the only delivery option is caesarean section. Use of an oxytocin infusion may be indicated in nulliparous women with inefficient uterine activity but extreme caution is required in the multiparous woman with secondary arrest or in women with a previous caesarean section, as attempts to overcome the obstruction of CPD with powerful uterine activity could result in uterine rupture, with all its consequences. In the second stage of labour, the operator must decide between attempted OVD and caesarean section, and if OVD is attempted the decision must be made on where to conduct the delivery and which instrument to use (32).
Failed OVD
In an ideal world, there would be no failed vacuum or forceps deliveries, only successfully completed OVDs and appropriately conducted second-stage caesarean sections. In the real world, the diagnosis of CPD is often unconfirmed until there has been an attempt to apply traction with a correctly positioned instrument during a contraction with maternal pushing. Some obstetricians choose not to do this and have abandoned mid-pelvic OVD entirely in favour of caesarean section (26, 42). Other obstetricians will attempt to apply their skills in appropriate circumstances with careful attention to a back-up plan should the attempt be unsuccessful (27, 37, 38).
The Royal College of Obstetricians and Gynaecologists (RCOG) guidelines emphasize that there should be progressive descent with each pull of a correctly applied instrument and that the total number of pulls should be limited (21, 43). With forceps delivery, it will be clear on the first or second pull whether or not CPD is relative or absolute and the delivery can be completed safely or abandoned accordingly. With vacuum extraction, the impression of descent can be more difficult to appreciate but certainly the procedure should be discontinued if the head has not reached the perineum by the third pull. Various studies have shown that a failed attempt at OVD in a setting where immediate recourse to caesarean section is available does not increase the maternal or neonatal morbidity and attempted mid-pelvic OVD will be successful in approximately half the selected cases (27, 38, 44). Nonetheless, every obstetrician should have a clear understanding of appropriate stopping rules and in the event of an abandoned attempt at OVD, the fetal head should be disimpacted to facilitate safe delivery by caesarean section.
Sequential instrument use
Vacuum extraction has become the instrument of choice in many settings and among the majority of obstetricians in training. This has important implications for the management of mid-pelvic arrest with a suspicion of relative CPD. In the prospective cohort study of women with complex deliveries transferred to theatre for arrested progress in the second stage of labour, attempted forceps was more likely to result in completed vaginal delivery than attempted vacuum (63% vs 48%; P process and where appropriate should be included in difficult consultations.
2. Consent: informed consent should be obtained from the woman after explicit counselling regarding the indication, benefits and risks, and nature of any procedures. Where possible, the birth plan/preferences of the mother should be taken into account and discussed. Verbal consent should be documented as a minimum but written consent is recommended for a ‘trial of instruments' in theatre or for caesarean section.
3. Documentation: it is essential that the indication for operative delivery, clinical assessment, conduct of the delivery, outcome for mother and baby, and consent process is documented clearly in the medical records. Particular attention should be paid to accuracy and consistency of recorded timings and to legibility of names and signatures. Paired cord blood samples should be processed and recorded in all cases. The use of a structured pro forma, such as the document recommended by the RCOG, reduces the likelihood of incomplete documentation but is not a substitute for documenting the decision-making process (21). The findings at caesarean section and after a failed attempt at OVD should be clearly recorded to inform the decision-making process for future births.
4. Outcome recognition: complications will occur and most prospective parents recognize this. However, failure to recognize that a complication has occurred results in anger, upset, complaints, and in some cases litigation. It is essential that obstetricians who perform complex operative deliveries have the skills to recognize and manage pelvic floor injuries and surgical complications. Neonates should be assessed by personnel with the expertise to recognize and manage brachial plexus injury, fractures, intra- and extracerebral haemorrhage, and the consequences of hypoxia.
5. Incident reporting: where adverse events occur, these should be reported through the local incident reporting procedures. Every unit should have a risk management structure in place to ensure that adverse events are dealt with in an appropriate and timely manner.