Malpresentation
Malpresentation refers to any presentation of the fetus other than vertex and includes face, brow and breech, shoulder or back presentation with a transverse lie, and compound presentations with more than one part presenting.
The most commonly encountered malpre- sentation is breech which is discussed in detail in Chapter 33. A firm application of the fetal presenting part on to the cervix is necessary for good progress in labour. A face presentation applies poorly to the cervix and the progress in labour may be slow, although vaginal birth is still possible. Brow presentation is associated with the mentovertical diameter presenting, which is simply too large to fit through the bony pelvis unless flexion occurs to a vertex presentation or hyperextension to a face presentation (Figure 32.1). Brow presentation therefore often manifests as poor progress in the first stage of labour, typically in a multiparous woman. Malpresentations relating to an abnormal or unstable lie are often diagnosed and managed prior to the onset of labour. Shoulder presentation cannot deliver vaginally and poor progress will occur if labour proceeds, together with an increased risk of arm or cord prolapse and uterine rupture.Aetiology
Malpresentations are more common in women of high parity, presumably due to laxity of the uterine muscle and abdomen. They are more common with polyhydramnios and extremes of fetal size, and with multifetal pregnancy (1, 2). They may occur as a result of a uterine malformation such as a bicornuate uterus or uterine septum or in the context of an abnormally located placenta. They may occur as a result of a fetal congenital abnormality such as anencephaly.
Diagnosis
The lie and presentation of the fetus should be determined in the first instance by clinical assessment using the standard approach of inspection, palpation, and auscultation.
A transverse or oblique lie and breech presentation should be readily detectable or suspected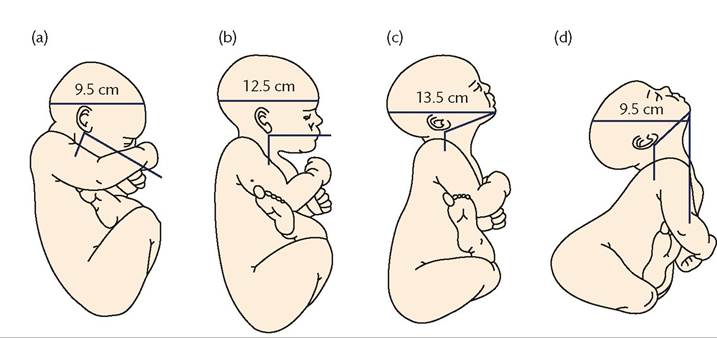
Figure 32.1 Fetal skull dimensions. (a) Flexed vertex presentation—suboccipitobregmatic diameter 9.5 cm. (b) Deflexed Occipitoposterior position- occipitofrontal diameter 11.5 cm. (c) Brow presentation—mentovertical diameter 13.5-14.0 cm. (d) Face presentation—submentobregmatic diameter 9.5 cm.
Reproduced from KP Hanretty, Obstetrics Illustrated, 7e., Churchill Livingstone 2009, with permission from Elsevier.
clinically. The findings can be confirmed by ultrasonography which has a higher sensitivity and specificity than clinical assessment alone (3) (Table 32.1). A clinical diagnosis of face or brow presentation is usually only suspected for the first time in labour. With a brow presentation, the fetal head may palpate as unengaged abdominally and the orbital ridges and bridge of the nose will be felt on digital vaginal examination with a prominent anterior fontanelle. Abdominal examination of a face presentation may be unremarkable but on digital vaginal examination the orbits, nose, and mouth will be felt with no palpable sutures. It may take a minute or two to differentiate a face presentation from a breech presentation.
Table 32.1 Use of ultrasonography for fetal assessment in labour
| Indication | I Evidence summary |
| Confirm presentation | |
| Singleton preterm | Accepted practice |
| Multiple pregnancy (especially twin 2) | Accepted practice |
| Clinical uncertainty | Observational data |
| Estimate fetal weight/gestational age | |
| Unbooked patient | Mainly observational data |
| Threshold of viability/preterm | Accepted practice |
| Suspected small fetus | Accurate for low birth weight |
| Suspected large fetus | Inaccurate for macrosomia |
| Fetal head in the first and second stage of labour | |
| Engagement and station | Limited data with different techniques used |
| Descent | Limited data with different techniques used |
| Position | Observational and RCT data |
| Cord abnormalities | |
| Nuchal cord | Limited data |
| Vasa praevia | Case reports |
| Placenta | |
| Placental location | Accepted practice |
The partogram may give important diagnostic clues.
In nul- liparous labour there may be primary arrest or slow progress despite good contractions. In multiparous labour, a secondary arrest or arrest in the second stage of labour warrants early assessment by an experienced obstetrician due to the increased risk of uterine rupture (Figure 32.2). In any of these circumstances, the possibility of a breech, face, or brow presentation should be considered. Ultrasonography may also be helpful in confirming the findings.Prevention
External cephalic version is the accepted approach to preventing breech presentation in labour. The options for preventing face, brow, shoulder, or compound presentations are less clear and encompass watchful waiting and timely rupture of membranes (4). With a transverse or oblique lie it is usually best to wait until full term or until the lie and presentation have stabilized prior to considering delivery. More than half will convert to a longitudinal lie and cephalic presentation with expectancy (5). Some obstetricians will offer a stabilizing induction of labour with preparations in place in case of cord prolapse or procedural failure requiring immediate caesarean section. Delayed decision-making with a transverse or oblique lie in labour can result in an arm, cord, or compound presentation that might have been prevented by a more timely decision for a caesarean section (Figure 32.3).
In terms of preventing a face or brow presentation, it is best to avoid rupturing the membranes with a high fetal head as the process of flexion takes place during descent of the presenting part within the pelvis. Mobilization, upright positions, and use of a birthing ball may encourage descent in these circumstances. Similarly, for a second twin it is best to wait for the fetal head to descend well into the pelvis prior to rupturing the membranes if a brow, face, or a compound presentation is to be avoided. An oxytocin infusion may facilitate this process.
Management
Face presentation
The incidence of face presentation is approximately 1 in 500 to 1 in 600 births.
The presenting diameter is the submentobregmatic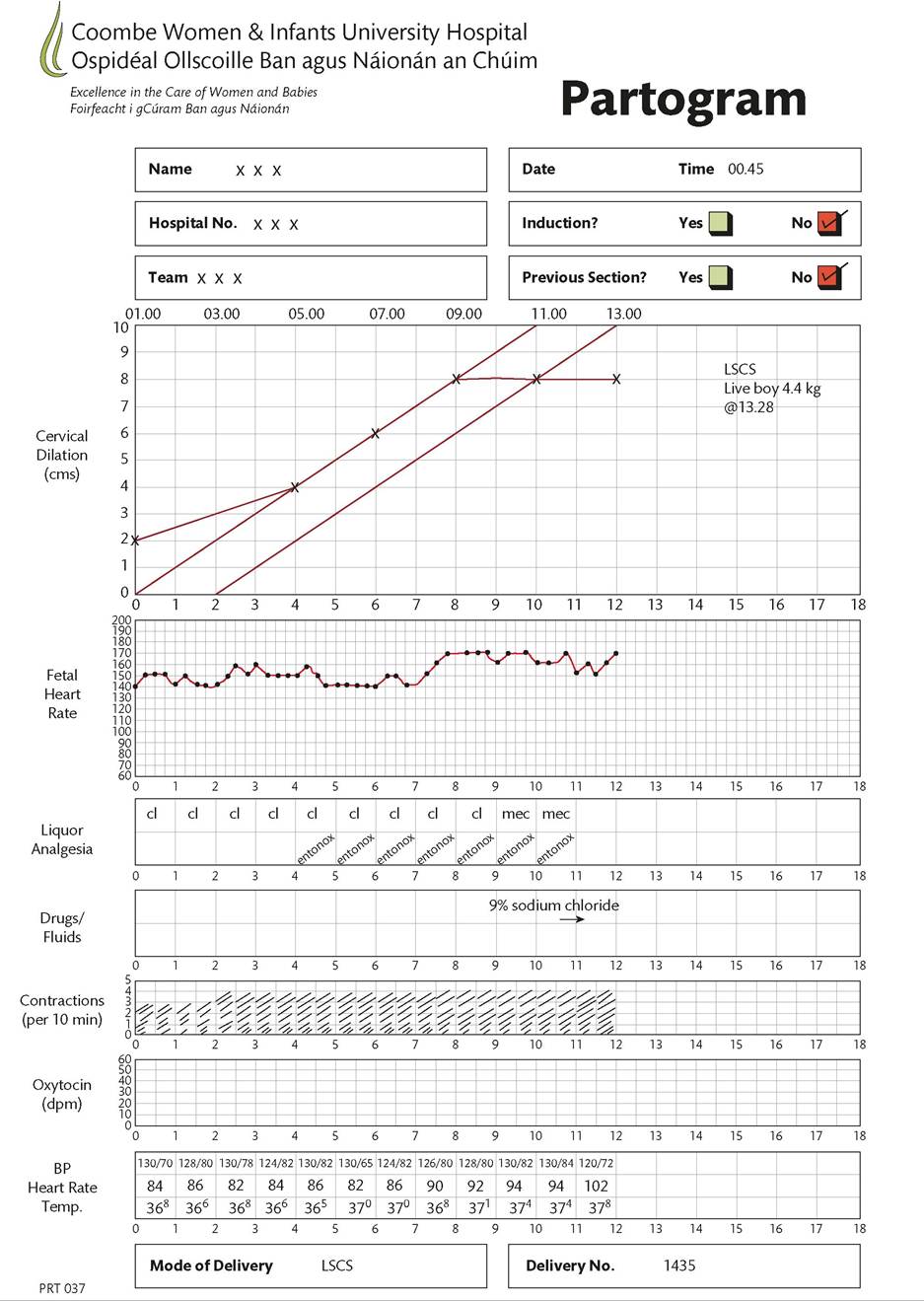
Figure 32.2 Partogram demonstrating secondary arrest in labour.
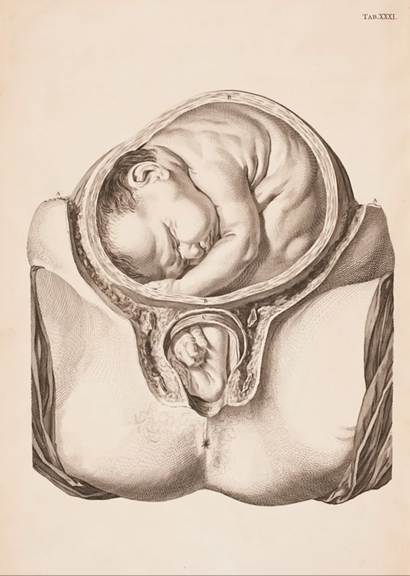
Figure 32.3 Compound presentation (transverse lie).
RCOG Library.
which measures 9.5 cm, similar to a vertex presentation, and as such the labour may not differ greatly from vertex labour (6). Expectancy is the usual approach aiming for a spontaneous vaginal delivery. The mother should be warned that the baby's face may be swollen or bruised at the time of birth but should revert to normal over the following days. The fetal head needs to rotate to a mentoanterior position for vaginal delivery to be achieved. Forceps delivery can be used in a mentoanterior position applying the same safety criteria as for vertex deliveries (Figure 32.4). Fetal blood sampling, fetal scalp electrodes, and vacuum extraction are contraindicated. If the position remains mentoposterior, delivery should be by caesarean section as it is not possible for the fetal head to extend further into the sacrum to allow delivery of the chin (7).
Brow presentation
The incidence of brow presentation is approximately 1 in 700 to 1 in 1000 births. The presenting diameter is the mentovertical which measures 13.5-14.0 cm in term fetuses and usually exceeds the capacity of the pelvis. In most cases this will result in arrested progress in the first stage of labour and delivery by caesarean section. If diagnosed in early labour, expectancy may result in flexion to a vertex presentation or complete extension to a face presentation, both of which may result in vaginal delivery. However, arrested progress in multiparous women and in women with a previous caesarean section requires particular caution as continuing with labour in the context of obstruction could result in uterine rupture.
Some authors report success with manual rotation from brow to vertex presentation at full dilatation with a high rate of vaginal delivery (8). This should only be performed by experienced obstetricians under regional anaesthesia and with immediate access to an operating theatre.Back or shoulder presentation
It is not possible for a term baby in a back or shoulder presentation to deliver vaginally and an early decision should be made to perform a caesarean section if labour starts. Caesarean section for a transverse lie is challenging, particularly with the fetal back down, and requires manipulation of the fetus in order to grasp a leg, aiming to deliver as a breech. This may result in extension of the uterine incision with maternal haemorrhage and/or trauma to the fetus (9). It is one of the potential indications for a classical caesarean incision.
Some authors report success with external version using tocolysis in the intrapartum management of the transverse lie (10). The success rate of conversion to a cephalic presentation is high (75%) but the caesarean section rate in labour is higher than that of vertex presentation from the outset. Nonetheless, caesarean section may be avoided in half the cases where external version is attempted. Internal podalic version in labour is associated with an increased risk of uterine rupture and should be avoided (11). Very preterm fetuses at the limits of viability may present with the back or shoulder deep in the pelvis at full dilatation and gentle manipulation to a cephalic presentation may result in spontaneous vaginal delivery rather than a technically challenging and potentially traumatic caesarean section.
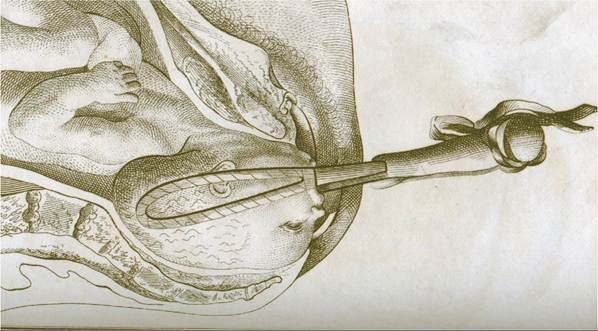
Figure 32.4 Face presentation-mentoanterior forceps delivery.
RCOG Library.
Compound presentation
Compound presentation occurs more commonly with preterm labour, vaginal delivery of a second twin, or with an abnormal lie (Figure 32.3). There may be a fetal head or breech presenting together with an arm or leg, or the cord may present alongside the presenting part. At full cervical dilatation, it may be possible to manipulate the fetus or await descent of the fetal head/breech, and vaginal delivery can be achieved. In term pregnancies, a fetal hand may be palpated alongside the fetal head in the first stage of labour. In the first instance this can be managed expectantly and in many cases the hand will retract as labour progresses and the larger head descends. In some cases, the arm may prolapse through the cervix in which case an urgent caesarean section needs to be performed. These deliveries require advanced obstetric skill in terms of both decisionmaking and operative delivery.