Management of women with uncertain early pregnancy diagnosis
Serial serum hCG measurement at an interval of 48 hours is useful in the management of women with a PUL. Most women are suitable for outpatient management because they are haemodynamically stable and therefore return home between visits for measurement of serum hCG concentrations.
Clear advice has to be impressed upon each woman about follow-up, emergency contact numbers out of hours, and about which symptoms should alert her to seek medical help sooner than planned. Worsening of existing symptoms or experiencing symptoms suggestive of intraperitoneal bleeding warrants an urgent review.A viable intrauterine pregnancy would be expected to be associated with at least a 66% increase from initial serum hCG concentration over 48 hours. The approximate doubling of hCG with healthy pregnancy is a predictable feature in the first trimester. An EP can be associated with a rise of less than 66% or a largely static serum hCG concentration. A 50% drop in serum hCG concentration over 48 hours is strongly suggestive of miscarriage, and associated vaginal bleeding with the passing of the sac through the cervix would further support this.
A stable woman with a serum hCG concentration below the discriminatory zone and PUL on TVUS scanning can safely have serial hCG monitoring. A second serum hCG concentration can suggest a diagnosis based on the hCG trend and if the subsequent serum concentration is above the discriminatory zone, a further TVUS scan may be helpful. Serum hCG concentrations for normal intrauterine pregnancies at equivalent gestation have a wide range. The individual trend in serum hCG concentrations is more useful in establishing a diagnosis and the absolute serum concentration is useful in interpretation of scan findings and subsequent decisions on management options. A normally developing intrauterine pregnancy will approximately double the serum hCG concentration every 48 hours.
A rise of more than 66% from the baseline is acceptable. This can roughly predict when a normal intrauterine pregnancy should be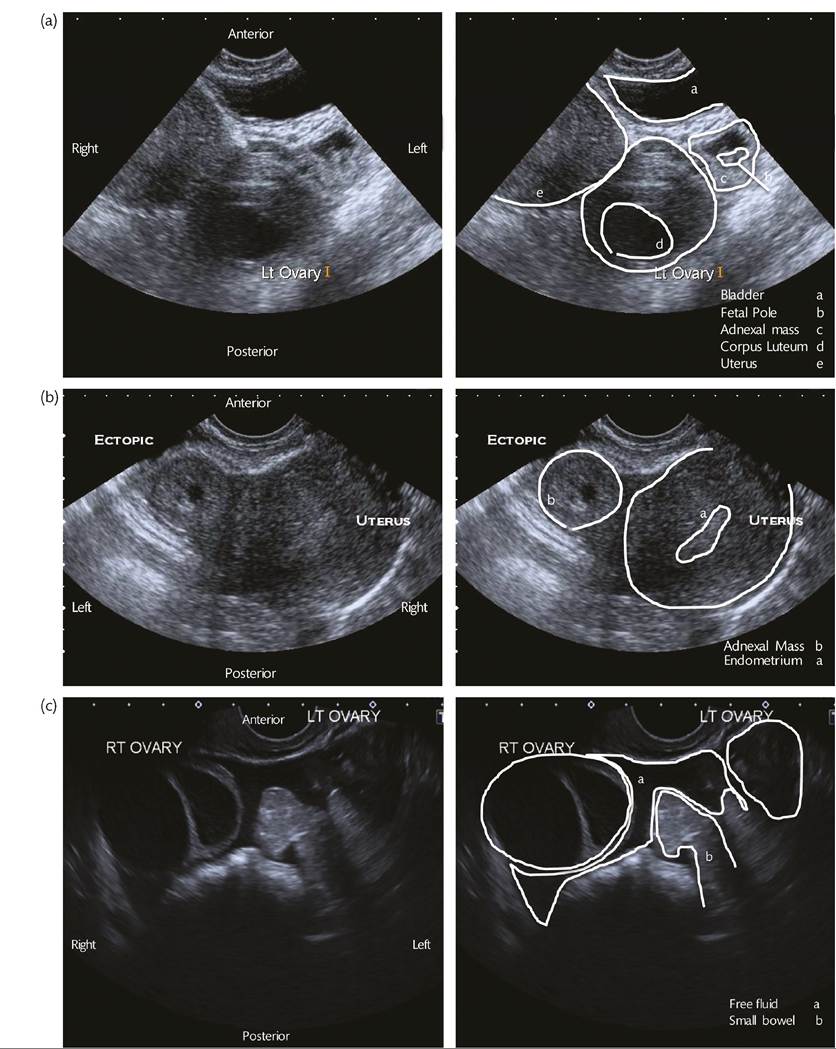
Figure 39.3 Ultrasound scan findings of (a, b)an empty uterus and either identification of an adnexal gestation sac, or a heterogeneous adnexal mass; panel (c) shows free fluid with floating small bowel taking the irregular shape of the pelvis and pouch of Douglas.
above the discriminatory zone and hence located on an ultrasound scan. This would be able to confirm the location of the pregnancy, and some cases confirm the presence of fetal heart motion. Some women may require a further scan to assess viability of the pregnancy, usually after at least 1 week. Once the pregnancy is located by ultrasound, serum hCG concentrations are of little value in determining viability or predicting pregnancy outcome.
A sharp fall in serum hCG concentrations from initial baseline within 48 hours with bleeding symptoms can allow a confident clinical diagnosis of miscarriage and further scans can be avoided. As the location of the pregnancy had never been confirmed, there is a small remaining possibility of an EP. This small risk is usually mitigated by ensuring follow-up of the women clinically and with serum hCG concentration. In addition, women are advised to re-attend if pain or bleeding worsens, if there are symptoms of intraperitoneal bleeding as described previously, or in those without ongoing contraception if their periods do not resume.
Serial hCG monitoring with PUL can result in the situation where there are several hCG results at 48-hour intervals, all below the discriminatory zone, neither clearly resolving nor doubling. These are

known as ‘persistent PULs' and either represent an underlying EP or a miscarriage, with the static pattern of the hCG not being consistent with a viable pregnancy.
A developing adnexal mass may become apparent in women with a PUL, which would strongly suggest an EP whether the corresponding serum hCG concentration is above or below the discriminatory zone. In those without an adnexal mass visible on ultrasound, taking a conservative approach with close monitoring should see the serum hCG concentration return to normal. Each woman with a PUL should be aware of the possibility of an EP and receive clear advice about action to take if symptoms worsen. Intraperitoneal bleeding is possible even at very low serum hCG concentrations so women and healthcare staff should remain vigilant for complications until the pregnancy has resolved and this has been confirmed by serum hCG concentrations (e.g. decrease to the woman prior to surgery regarding her wishes. A salpingectomy is indicated if the woman has no future desire for fertility, because of fewer surgical complications and less follow-up requirements. If the other fallopian tube and the rest of the pelvis appear healthy, the reproductive outcomes are similar with salpingectomy or salpingotomy (20).A salpingotomy is required if the woman wishes to conceive naturally in the future and the contralateral tube appears to be unhealthy, damaged, or absent. This could result from previous infection, surgery, endometriosis, or previous EP. There are equivalent reproductive outcomes after salpingectomy or salpingotomy. It can be difficult to know if all the pregnancy tissue has been removed when performing a salpingotomy, so follow-up serum hCG concentration monitoring is essential until the final resolution. There is an estimated 4-8% risk of residual trophoblast cells in the treated fallopian tube, which can multiply and cause further bleeding. A decrease
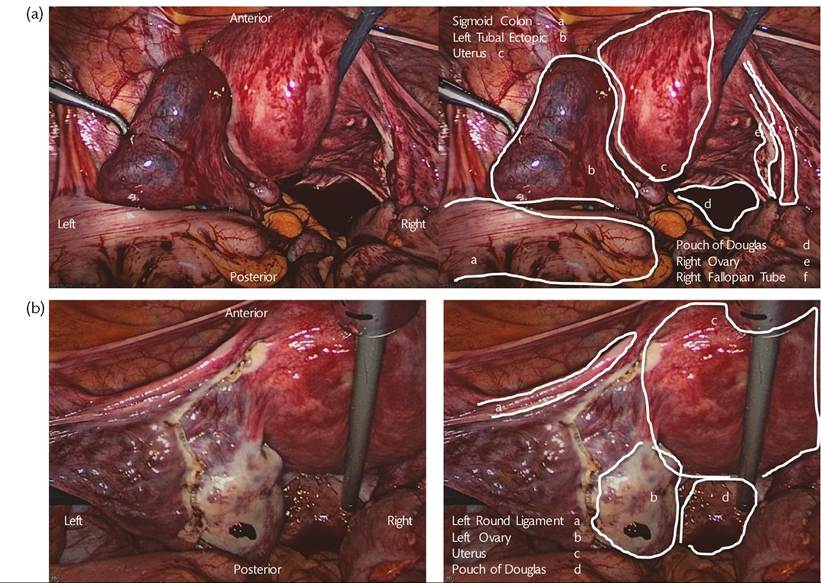
Figure 39.4 (a) The peritoneal cavity is filled with carbon dioxide gas to lift the anterior abdominal wall away from the abdominal viscera either before or after insertion of the camera, and direct visualization of the pelvis can be made.
(b) Other 5-10 mm incisions are made in the abdominal wall to allow surgical instruments to reach the pelvis and perform the necessary surgery.then a subsequent increase in the serum hCG concentration would alert healthcare staff to this possibility. This would require either a second operation to perform a salpingectomy or medical treatment. The risk of recurrent EP following a salpingotomy is 8% with an approximately even distribution between ipsilateral and contralateral tube as the future implantation site (20).
In women who are undergoing IVF-ET, there are further considerations for the surgeon to take into account. It is known that the presence of hydrosalpinges (abnormal fallopian tubes distended with fluid) increases the risk of embryo implantation failure and miscarriage, and that removal of the affected hydrosalpinges, or blocking the fluid from entering the uterine cavity with sterilization clips, reverses this (21). At laparoscopy for EP, a salpingectomy may be used to treat the EP, with contralateral tubal occlusion or contralateral salpingectomy (22). This would mean the chance of spontaneous conception in the future would be almost zero and that IVF would be needed for future pregnancies. The benefits in improved IVF success rate and reduced chance of future EP have to be carefully balanced and discussed with the woman and her fertility team in advance of surgery. If there is doubt or the findings at laparoscopy are unexpected, a conservative approach should be taken.
Surgery for EP is considered a potentially sensitizing event in the United Kingdom in rhesus-negative blood group women without prior sensitization, so 250 IU of anti-D immunoglobulin via intramuscular injection is recommended.
Medical management
This is an option for selected haemodynamically stable women with a suspicion of EP on ultrasonography or a persistent PUL. It can be a reasonable option when the woman and the gynaecologist wish to avoid laparoscopy.
There is no role for medical management in women with severe abdominal pain or suspicion of intraperitoneal bleeding. In either case, expedient surgery is more appropriate.Methotrexate is widely used for medical management of EP. It is usually given in a single intramuscular injection with a dose of 50 mg/m2 body surface area. Methotrexate is a systemic treatment that works by inhibiting dihydrofolate reductase (23). This interrupts the supply of substrate for synthesis of purine DNA base pairs. The downstream effect is to disrupt the cell cycle by preventing duplication of DNA. The effect of methotrexate is concentrated on cells dividing rapidly such as trophoblasts. Systemic methotrexate would disrupt trophoblast cells sited in an EP or in an intrauterine pregnancy equally, so the presence of an intrauterine pregnancy is a contraindication for medical management. The teratogenic nature of methotrexate means a 12-week washout period is recommended before a further attempt to conceive. The common side effects of methotrexate are related to the effect of rapidly dividing cell disruption in the skin, bone marrow, and gastrointestinal tract, namely photosensitivity, leucopenia, stomatitis, and diarrhoea. Women treated with methotrexate maintain their oocyte reserve when it is used as a single dose in this manner, emphasizing the effect on actively dividing rather than quiescent cells (24).
Patient selection for medical management is important. Methotrexate has been successfully used in women with a baseline serum hCG concentration less than 5000 IU/L. Above this level, the frequent resort to surgery, or multiple doses of methotrexate, result in it being considered ineffective and not cost-effective (25). Mirroring criteria for surgical management, women best suited for methotrexate have an adnexal mass less than 35 mm in diameter, without the presence of fetal heart motion in the mass, and at most a small amount of free fluid on ultrasonography. In this context, a small amount of free fluid is considered within normal limits, whereas a moderate or large amount of free fluid would suggest intraperitoneal bleeding.
It may be useful in avoiding surgery in women at high risk of surgical complications, such as those with multiple previous abdominal surgeries, provided other requirements are met.When used as part of the management of persistent PUL, the aim of medical management is to accelerate or promote the complete resolution of the trophoblast. Until this happens and is confirmed by serum hCG concentration, the risk of intraperitoneal bleeding remains. In persistent PUL, the true diagnosis lies between EP and miscarriage. Around 20% of cases of persistent PUL are subsequently discovered to be EPs. Small EP masses can remain undetected by laparoscopy with both fallopian tubes appearing healthy without distention. It is justifiable to treat persistent PUL with methotrexate, and specific management can otherwise be offered should the underlying diagnosis become apparent with subsequent investigations.
Due to the side effect profile of methotrexate, a baseline full blood count, liver function tests, and renal function should be measured alongside serum hCG. Abnormalities in these parameters are likely to be worsened by methotrexate and an alternative to methotrexate should be considered.
Women treated medically are typically managed as an outpatient. Clear advice about symptoms that suggest intraperitoneal bleeding and how to access care swiftly are essential. To facilitate this safely, the woman should have 24-hour access to emergency gynaecology care including resort to urgent surgical management and be able to attend hospital promptly if her symptoms worsen.
After the initial injection, close monitoring is required until the serum hCG concentration is negative. This can take several weeks and women should be prepared to have regular measurement of serum hCG concentrations as part of medical management. Initial response to methotrexate is determined by checking serum hCG concentrations at 4 days and 7 days after the injection. A result showing a greater than 15% decrease in serum hCG concentration when comparing these serum concentrations is indicative of a good initial response. Serum HCG concentrations are checked weekly thereafter to ensure a continuing decrease until complete resolution is achieved. Some units consider medical management a potentially sensitizing event and will offer anti-D immunoglobulin at the same dose for surgical management to unsensitized rhesus negative women.
Between 80% and 90% of women with an EP treated with methotrexate will have successful treatment, meaning surgery or further methotrexate have been avoided. Around 10% of appropriately selected women will required either a second dose of methotrexate or surgical management, both indicating a suboptimal response to medical management. This may become apparent with a worsening of symptoms with clinical or ultrasound suspicion of intraperitoneal bleeding mandating surgical treatment. Alternatively, the woman may no longer wish to continue with medical management. Serum concentrations of hCG after methotrexate which have risen on day 7 give an early indication to move to surgical management. During the serum hCG follow-up phase, the concentrations may plateau or begin to rise again before any symptoms are reported from the woman, indicating failing medical management and giving an opportunity to consider surgical management prior to any clinical deterioration. The risk of intraperitoneal bleeding remains for the woman until the resolution of serum hCG is complete. The risk of recurrent EP after successful medical management is 12%, similar to that after surgery (26).
Expectant management
Careful selection of woman can identify those in whom the EP will resolve spontaneously, avoiding the risks associated with surgical and medical management.
The general characteristics in favour of successful expectant management are a low initial serum hCG concentration, usually less than 1000 IU/L with a downward trend (27). Otherwise the criteria are similar to those required for outpatient medical management.
Serum hCG concentration is monitored at a minimum of weekly intervals until negative, taking an average of less than 3 weeks (14, 28-30). As with methotrexate treatment follow-up, a plateau or rise in serum hCG concentration during monitoring can trigger alternative forms of management to be offered to the woman. Easy access to gynaecology care is essential.