Diagnosis and managing uncertainty
Haemodynamically unstable women with a positive pregnancy test can be assumed to have a bleeding EP. They require urgent intervention and circulating volume replacement. There is no alternative.
The diagnosis in haemodynamically stable women in early pregnancy is commonly made by ultrasonography, supported by quantitative serum hCG concentration. The three most common eventual outcomes are of a viable intrauterine pregnancy, non-viable intrauterine pregnancy (commonly referred to miscarriage), and EP. Knowledge of how the diagnosis is made for each is essential in understanding EP.
A transabdominal ultrasound scan is sometimes performed first. The woman requires a full bladder in order to obtain high-quality images. The full bladder facilitates the transmission of ultrasound waves between the body tissues and the transducer (probe) on the skin. The uterus, ovaries, and bladder can be assessed as well as more distant areas as needed such as kidneys and appendix.
A transvaginal ultrasound (TVUS) scan is used to image the uterus, ovaries, and pelvis with higher resolution. This requires the woman's consent, and privacy for her to empty her bladder and to undress. 'The transvaginal probe is covered in ultrasound gel, a probe cover, and lubricating gel. The probe is inserted into the vagina and the tip gently placed at the posterior fornix of the vagina—better resolution is obtained because the uterus and ovaries are closer to the transducer at the probe tip.
As an embryo implants and begins to grow in size it will at some point cause changes which are detectable by ultrasound. These changes occur long before any changes which would be detected by findings on clinical examination. Deviation from the progression of ultrasound findings in a normally developing intrauterine pregnancy would strongly suggest an alternative pregnancy outcome.
Figure 39.1a shows a normal-sized uterus with a thin endometrium as expected in the non-pregnant female. Figure 39.1b shows a thickened endometrium in keeping with secretory phase endometrium or very early stages of pregnancy. The embryo if present is too small to be seen by modern ultrasound machines. Figure 39.2a shows a small sac in the endometrial cavity, which is located towards one side of the cavity. This is known as an eccentrically placed sac and is suggestive of an intrauterine pregnancy. This stage falls short of confirmation that the pregnancy is developing in the uterine cavity. The reason for this is because the sac appears empty, that is, without any other structures visible within it. An empty sac placed centrally in the uterine cavity is a ‘pseudosac' and is likely to be a small collection of blood pooling in the uterine cavity.
Pseudosacs are associated with EPs, and if misinterpreted can falsely reassure a woman with an EP that the pregnancy is intrauterine. Figure 39.2b shows an intrauterine sac with a yolk sac. The presence of the yolk sac means that the whole intrauterine sac can now be referred to as a gestation sac. This finding means that the pregnancy is intrauterine. The stage of development is in keeping with normally developing pregnancy. A follow-up scan is required
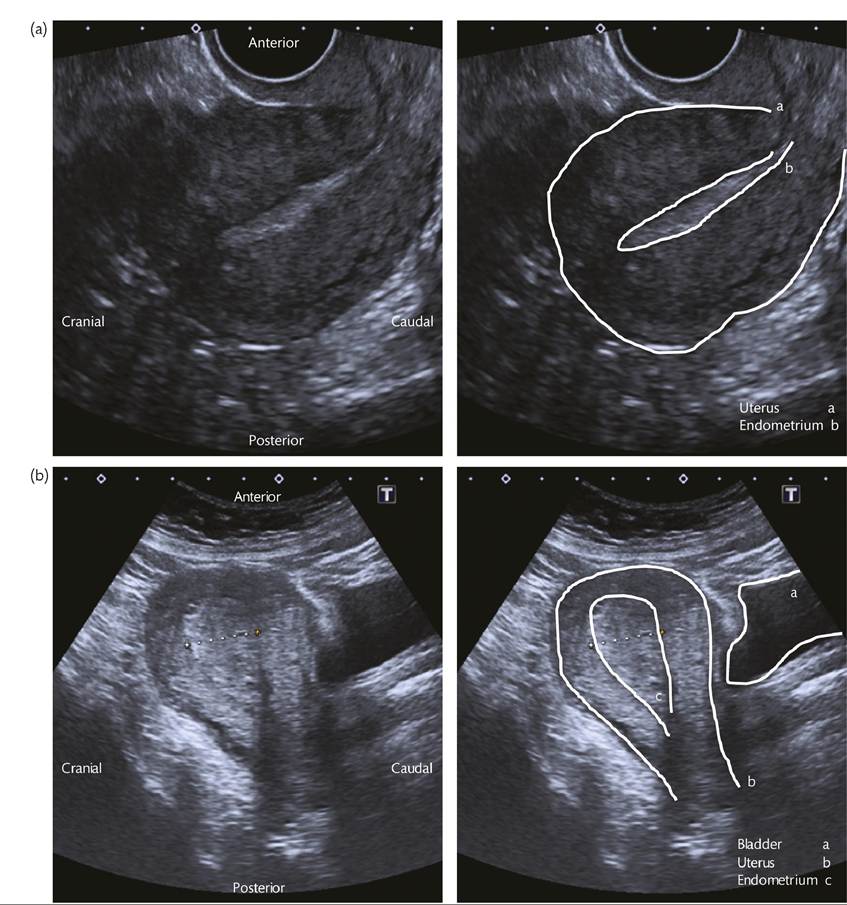
Figure 39.1 Ultrasonography shows (a) a normal-sized uterus with a thin endometrium as expected in the non-pregnant female, and (b) a thickened endometrium in keeping with secretory phase endometrium or very early stages of pregnancy.
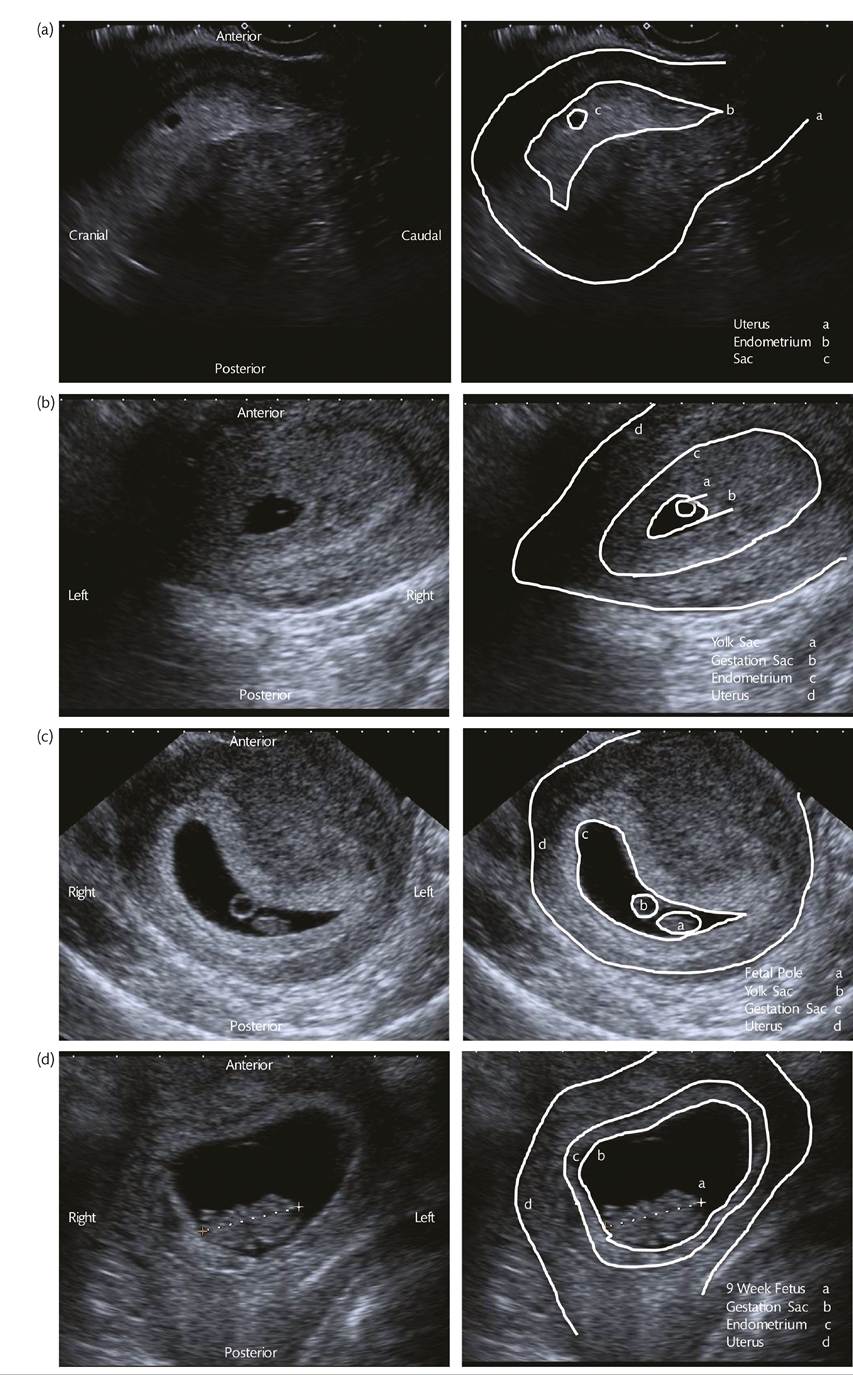
Figure 39.2 Ultrasonography shows (a) a small sac in the endometrial cavity, which is located towards one side of the cavity, and (b) an intrauterine sac with yolk sac. The presence of the yolk sac means that the whole intrauterine sac can now be referred to as a gestation sac; (c) a follow-up scan.
Panel (d) shows a developing fetus of 9 weeks' gestation within the uterus with fetal heart motion and fetal movements seen clearly during the scan.as shown in Figure 39.2c to confirm or refute viability. An additional structure, the fetal pole, is now seen in the gestation sac. Using a TVUS scan under ideal conditions, fetal heart motion can be seen when the fetal pole measures 2-3 mm in length, and this would confirm viability. The absence of fetal heart motion with a small fetal pole may suggest miscarriage; however, it may be in keeping with very early stages of a normal pregnancy also. A repeat scan at least 7 days apart should reveal further development in the size of the gestation sac and fetal pole with fetal heart motion now visible confirming a viable pregnancy. The absence of development, the absence of fetal heart motion with a fetal pole greater than 7 mm (in the United Kingdom), or an empty uterus with a thin endometrium suggest a non-viable pregnancy (1). Guidelines for making the diagnosis of miscarriage are designed to minimize the risk of inadvertently reporting an early-stage viable pregnancy as non-viable (1). The absence of a previously seen gestation sac in association with a history of vaginal bleeding strongly suggests that a miscarriage has occurred between scans and the fetal tissue has been passed through the cervix. Figure 39.2d shows a developing fetus of 9 weeks' gestation within the uterus with fetal heart motion and fetal movements seen clearly during the scan.
As described previously, there is a point during the normal growth of a viable intrauterine pregnancy in which the developing structures can be detected by ultrasound. This will vary between women and pregnancies. In women with technical obstacles to ultrasound such as a retroverted uterus, fibroids, or obesity, the healthy pregnancy will only be detected at a more advanced stage when larger structures are present. This will also be the case for women in whom only a transabdominal ultrasound scan is acceptable.
Correlation of inconclusive scan findings with the serum hCG concentration have led to the development of the concept of the ‘discriminatory zone' (12). This is the serum hCG concentration above which a normally developing and normally sited pregnancy should always be visible on ultrasound imaging. The use of TVUS scanning and improvement in the ultrasound technology mean that under optimal conditions this is between serum hCG concentration of 1000 and 1500 IU/ L (13). This means that inconclusive scan findings in Figures 39.1 and 39.2 with a corresponding serum hCG concentration below the discriminatory zone can be in keeping with a healthy pregnancy. The same findings with a serum hCG concentration well above the discriminatory zone would raise concerns about miscarriage or EP. Once the pregnancy is confidently located by ultrasound, the serum hCG concentration adds very little to the information already obtained by ultrasound.Figure 39.2d demonstrates ultrasound findings with an intrauterine pregnancy with or without fetal viability. A repeat scan after 1-2 weeks is sometimes required to allow development to demonstrate viability, or to demonstrate the lack of development associated with miscarriage.
The presence of an EP can be strongly suggested by scan findings of an empty uterus and either identification of an adnexal gestation sac, or a heterogeneous adnexal mass as demonstrated in Figures 39.3a and 39.3b. TVUS scanning can have a positive predictive value of 97% and a negative predictive value of 99% in diagnosis of EP in experienced centres (14). The presence of a small or trace amount of free fluid in the pelvis is common in early pregnancy scanning. A large amount of free fluid in the context of a suspected EP can be assumed to be blood, and will usually warrant surgical management. Figure 39.3c shows free fluid with floating small bowel taking the irregular shape of the pelvis and pouch of Douglas.
Of stable women presenting with symptoms in early pregnancy, typically 70% will have an intrauterine pregnancy identified at the initial scan.
Approximately half of those will have viability confirmed during the same scan, with the other half requiring further investigation or follow-up to reach a final diagnosis. About 10% of women will have a miscarriage diagnosed on the first scan, and around 2% depending on the local population will have an EP(15). The remainder will fall between the criteria described previously where the pregnancy sac cannot be identified either within or outside the uterus. This includes women with serum hCG concentrations above and below the discriminatory zone. The women are given the working diagnosis ‘pregnancy of unknown location' (PUL)
(16). This is an intermediate diagnosis for which further or repeat investigation is required to reach a final diagnosis or pregnancy outcome. This could be a viable intrauterine pregnancy, non-viable intrauterine pregnancy, or an EP. Around 20% of women initially classed as PUL will have an EP.
More on the topic Diagnosis and managing uncertainty:
- Diagnosis and managing uncertainty
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- FIVE COMPONENTS OF LEGAL COMPETENCIES