Maternal collapse
Maternal collapse is severe respiratory or circulatory distress that may lead to a sudden change in the level of consciousness or cardiac arrest if untreated. The possible causes of maternal collapse are listed in Figure 29.1 (6).
Signs of maternal collapse include:
• obstructed or noisy airway
• respiratory rate less than 5 or greater than 35 breaths per minute
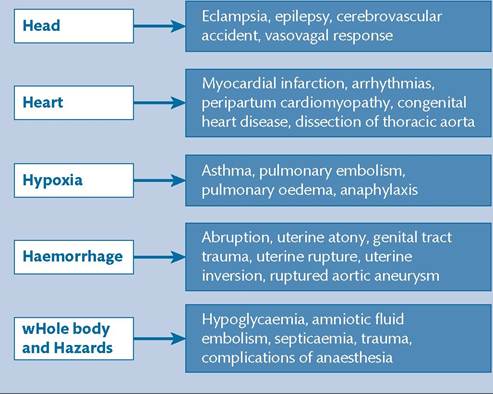
Figure 29.1 Possible causes of maternal collapse.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi-Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.
| Head | How responsive is the patient? Is she alert, responsive to voice, responsive to painful stimuli or unresponsive (AVPU)? Is the patient fitting? |
| Heart | What is the capillary refill like? What is the pulse rate and rhythm? Is there a murmur? |
| Chest | Is there good bilateral air entry? What are the breath sounds like? Is the trachea central? |
| Abdomen | Is there an 'acute' abdomen (rebound and guarding)? Is there tenderness (uterine or non-uterine)? Is the fetus alive? Is there a need for a laparotomy or delivery? |
| Vagina | Is there bleeding? What is the stage of labour? Is there an inverted uterus? |
Figure 29.2 A primary obstetric survey.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi-Professional Training.
Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.• heart rate less than 40 or greater than 140 beats per minute (bpm)
• blood pressure less than 80 or greater than 180 mmHg
• sudden decrease in level of consciousness
• unresponsive or responding to painful stimuli only
• seizures.
Initial management should follow the same basic principles of management of any critically unwell patient; call for help and assess airway, breathing, and circulation (ABC). If there are no signs of life, commence basic life support, as per United Kingdom Resuscitation Council Guidelines (9). Manually displace the uterus to the left to reduce aortocaval compression from the gravid uterus. Alternatively, this can be achieved with a 30-degree tilt if on a firm surface (e.g. theatre table).
If there are signs of life, place the woman in the recovery position and administer high-flow oxygen. Obtain intravenous access and send blood samples for full blood count, group and save, glucose, urea and electrolytes, liver function tests, and clotting screen. Check vital observations: blood pressure, heart rate, respiratory rate, oxygen saturations, and temperature. Establish continuous monitoring if possible. Perform an electrocardiogram. Commence intravenous fluids, providing there are no obvious contraindications (e.g. eclampsia).
After the initial management, perform a primary obstetric survey, as per Figure 29.2 (6).
If the diagnosis is not evident, consider key treatment decisions:
• Should the baby be delivered to improve maternal resuscitation?
• Is fluid resuscitation a priority? Are there any contraindications to fluids?
• Is the likely cause severe sepsis and therefore are intravenous antibiotics a priority?
• Is intensive care support required?
Once the woman is stable, perform a secondary obstetric survey to guide further investigations and management, as outlined in Figure 29.3 (6).
Resuscitation of a pregnant woman
Maternal cardiac arrest is rare, with a very high maternal and fetal mortality rate.
Although management follows the same principles of| ACTION | DETAIL |
| History | Revisit the history of the collapse and the previous history of the woman Read the notes and ask the partner or relatives |
| Examine | Repeat the examination going from top to toe |
| Investigate | Take arterial blood gases, troponins, blood glucose, lactate, blood cultures, ECG, chest X-ray, and ultrasound of the abdomen, high vaginal swab |
| Monitor | Continue monitoring of ECG, respirations, pulse, blood pressure and pulse oximetry Consider arterial and central venous pressure lines to aid monitoring |
| Pause and think further | Consider further investigations such as CT/MRI scans and echocardiography Ask relevant experts for their opinions |
Figure 29.3 A secondary obstetric survey. CT, computed tomography; ECG, electrocardiogram; MRI, magnetic resonance imaging.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi- Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.
basic and advanced life support, resuscitation of a pregnant woman is more difficult. There are several important factors to consider:
• When a pregnant woman is lying flat, the gravid uterus compresses the aorta and vena cava, decreasing venous return to the heart and resulting in up to 70% decrease in cardiac stroke volume. This will hinder resuscitation efforts, specifically the effectiveness of cardiopulmonary resuscitation (CPR). Aortocaval compression will be relieved by manual displacement of the uterus to the left or a 30-degree tilt on a firm surface.
• The baby should be delivered within 5 minutes of cardiac arrest, to aid maternal resuscitation. This will improve the effectiveness of CPR by removing the oxygen and circulating volume requirement of the fetus and placenta and by relieving aortocaval compression from the gravid uterus. Expediting the birth of the baby should be considered as soon as the woman arrests and the procedure should be commenced by 4 minutes if CPR is not successful. The baby should be born by the quickest means possible; often by caesarean section, although operative vaginal birth can be considered if the woman is fully dilated. CPR should be continued throughout the birth procedure. The neonatal team should also be summoned.
• Intubation is a priority. Aspiration of gastric contents is more likely due to hormonal relaxation of the oesophageal sphincter and delayed gastric emptying. Intubation can be more difficult because of oedema and the physiological changes of pregnancy causing a larger tongue and breasts.
• Ventilation is more difficult due to the increased intra-abdominal pressure from the gravid uterus.