Maternal sepsis
Maternal sepsis is the most common cause of maternal death in the United Kingdom (1). Although direct causes such as genital tract sepsis have decreased, there have not been any improvements in indirect causes such as pneumonia, urinary tract infection, breast abscess, and meningitis.
Between 2009 and 2012, the incidence of maternal deaths from direct and indirect causes of sepsis was 1.56 per 100,000 maternities (1).During this time period, almost a quarter of women who died had sepsis. Nearly 10% of women died from influenza. The influenza vaccine may have prevented more than half of these cases. Influenza vaccination for pregnant women is a public health priority.
Sepsis is defined as the presence of infection with systemic manifestations. Severe sepsis is defined as sepsis with organ dysfunction or tissue hypoperfusion. Septic shock is defined as sepsis-induced hypotension persisting despite adequate fluid resuscitation (10). Severe sepsis has a mortality rate of 20-40%, which increases to 60% if septic shock develops (11).
Sepsis is often insidious in onset. Pregnant women are usually young and fit, compensating well with infection until sudden cardiovascular decompensation. Presentation is often late, preceded by a short duration of illness and rapidly deteriorating into septic shock, disseminated intravascular coagulation, and multiorgan failure.
Recognition of sepsis
The clinical picture may not always reflect the severity of the underlying infection. The woman may just feel ‘not quite right' or may be unusually anxious or distressed. In antenatal women, an abnormal or absent fetal heartbeat may indicate sepsis. Postpartum women may have had a completely straightforward labour and no obvious risk factors. Observing trends in observations on MOEWS charts and performing a full clinical examination will help to identify women who have, or are developing, sepsis.
Risk factors
• Prolonged ruptured membranes
• Preterm labour
• Retained products of conception
• Caesarean birth
• Wound haematoma
• Cervical suture
• Invasive intrauterine procedure (e.g. amniocentesis)
• Obesity
• Impaired immunity
• Diabetes mellitus
• Working with, or having, young children.
Group A Streptococcus is the most common organism identified in maternal deaths from genital tract sepsis. Up to 30% of the population are asymptomatic carriers of this organism in their throat or skin. Streptococcal sore throat is one of the commonest bacterial infections of childhood. Spread is common via person-to- person contact and droplet spread. Symptoms can be non-specific and difficult to differentiate from less serious conditions such as gastroenteritis.
Symptoms of genital tract sepsis
• Abdominal pain
• Fever
• Diarrhoea
• Vomiting
• Offensive vaginal discharge
• Sore throat
• Upper respiratory tract infection
• Wound infection.
Signs of genital tract sepsis
• Rash: typically developing over 12-48 hours, initially appearing as blanching, erythematous patches on the chest and axillae, spreading to the trunk and extremities.
• Tachycardia greater than 100 bpm.
• Increased respiratory rate greater than 20 breaths per minute.
• Temperature less than 35°C or greater than 38°C (or a rise or fall in temperature).
• Systolic blood pressure less than 80 mmHg.
• Low oxygen saturations less than 95% on air.
• Poor peripheral perfusion: capillary refill greater than 2 seconds.
• Pallor.
• Clamminess.
• Confusion.
• Mottled skin.
• Low urine output less than 0.5 mL/kg/hour.
Initial management of maternal sepsis
An algorithm for the initial management of maternal sepsis is displayed in Figure 29.4.
Activate the emergency buzzer to call for urgent help from the multiprofessional team: senior midwives, obstetricians, and anaesthetists. Critical care consultants may also need to be involved in the woman's care.
Assess ABC and administer high-flow oxygen.Administer high-dose broad-spectrum antibiotics immediately, according to local antibiotic guidelines. Do not wait for laboratory blood results. Ideally send blood cultures prior to giving antibiotics, but do not delay the commencement of antibiotics.
Commence rapid fluid resuscitation. If the woman is hypotensive or has an elevated serum lactate of greater than 4 mmol/L, give at least 30 mL/kg of intravenous crystalloid, for example, a 70 kg woman should be given at least 2 L of Hartmann's solution (10). If the blood pressure or lactate level does not improve, consider transfer to an intensive care unit for vasopressors, to maintain the mean arterial pressure at greater than 65 mmHg. Women with septic shock often require aggressive fluid resuscitation. It is important to closely monitor fluid balance and for signs of fluid overload.
Full clinical examination
Perform a full clinical examination, including vaginal examination, to identify the cause of sepsis.
Send blood samples
• Full blood count: an increased or decreasing white cell count may be indicative of sepsis.
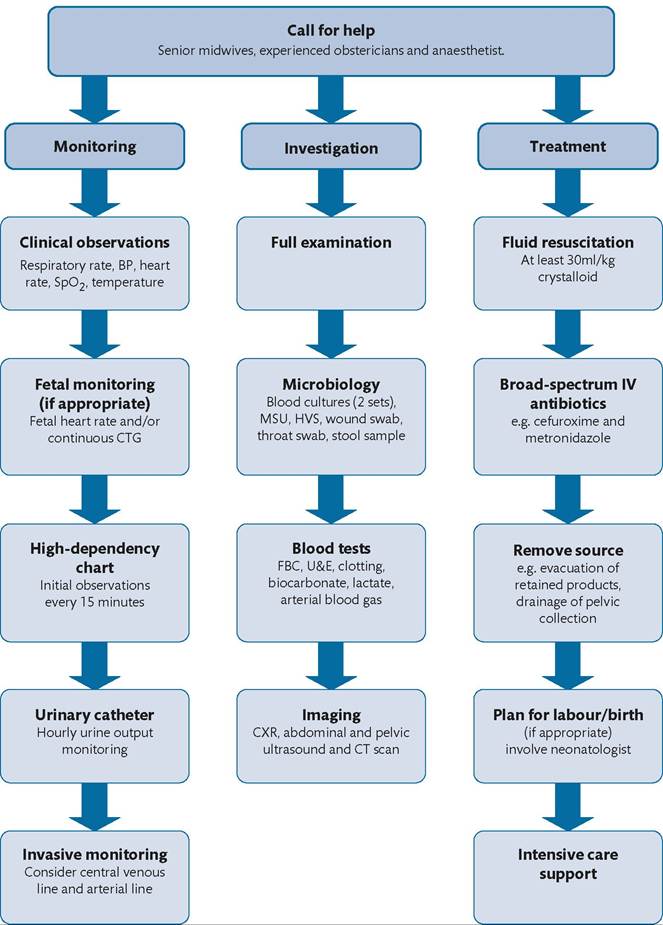
Figure 29.4 Algorithm for the initial management of maternal sepsis.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi-Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.
• C-reactive protein, urea and electrolytes, and liver function tests.
• Clotting screen (including fibrinogen): disseminated intravascular coagulation can arise as a result of severe sepsis. Clinical signs include undue bleeding or bruising.
• Lactate: a serum lactate concentration greater than 2 mmol/L signifies poor tissue perfusion secondary to severe sepsis or septic shock. A lactate level greater than 4mmol/L indicates a poor prognosis (12).
The lactate level is particularly useful for identifying women with tissue hypoperfusion who are at risk of septic shock but are not yet hypotensive or exhibiting obvious signs. An arterial blood gas analyser on the labour ward or in the neonatal intensive care unit will often be able to measure a serum lactate level from a venous or arterial blood sample.• Arterial blood gas: this will likely show metabolic acidosis due to the production of lactate and will worsen as shock progresses.
Send microbiology samples from all potential sources of sepsis
• Blood cultures
• Urine culture
• Vaginal swabs
• Placental swab (if applicable)
• Throat swab
• Wound swab
• Stool sample
• Sputum sample.
Remove the source of sepsis
If there are signs of chorioamnionitis, expedite birth and inform the neonatal team. Remove any retained products of conception once the woman is stable and after discussion with a senior obstetrician. Consider imaging: chest radiography, abdominal/ pelvis ultrasonography, and computed tomography of the chest/ abdomen/pelvis.