Phenotypes and staging of endometriosis
Phenotypes
Endometriosis can present as three different phenotypes: superficial endometriosis, deep endometriosis, and ovarian cystic endometriosis. Superficial or peritoneal endometriosis comprises superficial lesions scattered over the peritoneal, serosal, and ovarian surfaces.
Superficial endometriotic lesions or often divided in ‘typical’ blackbrown lesions and ‘atypical’ or ‘subtle’ lesions including red implants and clear vesicles (Figures 45.2 and 45.3). Ovarian cystic endometriosis refers to an endometrioma or ovarian cyst containing dark-stained blood (chocolate fluid) and lined by a pseudocyst wall covered by ectopic endometrium (Figures 45.4 and 45.5). Deep endometriosis, defined as endometriosis infiltrating more than 5 mm beneath the peritoneal surface, is a multifocal pathology that may infiltrate different organs (Figures 45.6 and 45.7). The most commonly affected sites are the intestine, vagina, uterosacral ligaments, bladder, and ureter but deep endometriosis is also occasionally observed in remote organs such as lymph nodes, umbilicus, and lungs (25). In women with deep endometriosis, intestinal and urinary tract involvement are estimated to occur in 3.8-37% and in 1-2%, respectively (26, 27).Deep endometriosis in the bowel is defined as ‘bowel endometriosis’ only if the muscularis layer is affected (26). Lesions with dense adhesions and/or endometriotic infiltration up to the bowel serosa are not considered bowel endometriosis, because these
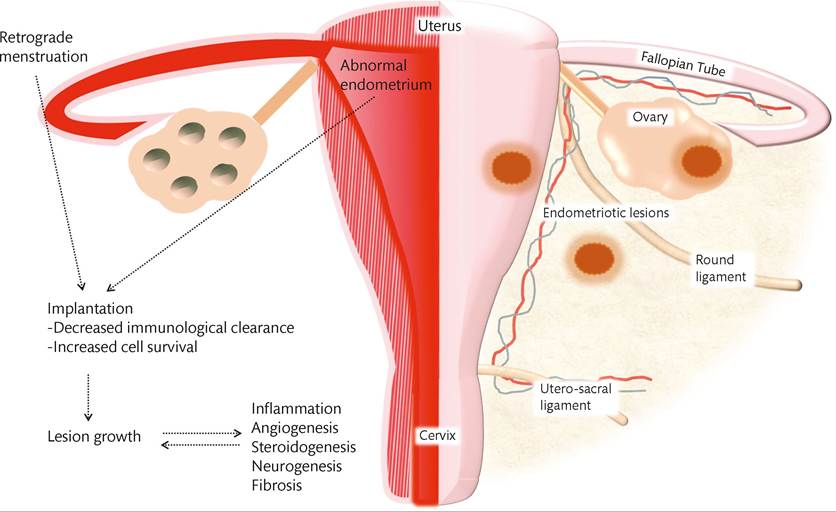
Figure 45.1 Overview of the pathogenesis of endometriosis. Courtesy of Dr Arne Vanhie
lesions are usually less than 5 mm in depth (28). The rectum and rectosigmoid junction together account for 70-93% of all intestinal endometriotic sites (26). In addition to the rectosigmoid junction, the most common intestinal sites are the appendix (218%), the distal ileum (2-16%), and the cecum (studies have tried to analyse the predictive value of certain symptoms in the diagnosis of endometriosis.
Overall, the evidence for the use of the ‘presence of symptoms' as an indication for the diagnosis of endometriosis is weak with low specificity and sensitivity (2). The European Society of Human Reproduction and Embryology (ESHRE) guideline on management of women with endometriosis states that the following symptoms and patient characteristics are risk factors for endometriosis: abdominopelvic pain, dysmenorrhea, heavy menstrual bleeding, infertility, dyspar- eunia, postcoital bleeding, a history of ovarian cyst, irritable bowel syndrome, and pelvic inflammatory disease (2). ESHRE also stated that the presence of multiple factors increases the chance of presence of endometriosis (2). In a prospective study, the presence of dyschezia during menstrual bleeding was a strong predictor for higher stages of endometriosis (ASRM stage III and IV) (46).Clinical examination can further increase the suspicion of presence of endometriosis and guide the planning of further imaging. However, the clinical examination has a low specificity and sensitivity for the diagnosis of endometriosis, especially peritoneal endometriosis, and clinicians should consider the diagnosis of endometriosis in women suspected of the disease even if the clinical examination is normal (2). There is evidence that the accuracy of the clinical examination is improved when performed during menstruation (47). Although clinical examination might be normal in many women with endometriosis, a routine inspection of the vagina using speculum, bimanual palpation, and rectovaginal palpation is recommended (2, 48, 49). Several studies emphasize the importance of inspection of the posterior fornix and rectovaginal digital examination for the diagnosis of infiltrating nodules of the vagina, uterosacral ligaments or the pouch of Douglas, as well as the detection of infiltration or masses in the rectovaginal septum and ovaries or displacement of the uterus or cervix (47, 48).

Imaging
Transvaginal ultrasound
Both ESHRE and the American College of Obstetricians and Gynecology (ACOG) recommend the use of TVUS in the diagnostic workup of women with suspected endometriosis (2, 50).
TVUS is useful in identifying endometriosis, however, the sensitivity and specificity of the examination are dependent on the interest and experience of the sonographer and on the quality of the ultrasound equipment (51, 52).In the recent Cochrane review by Nisenblat and colleagues, the sensitivity and specificity of TVUS for detecting ovarian endometriosis was 0.93 (95% confidence interval (CI) 0.87-0.99), and 0.96 (95% CI 0.92-0.99) respectively (39). For detection of deep endometriosis, the sensitivity and specificity of TVUS was 0.79 (95% CI 0.69-0.89) and 0.94 (95% CI 0.88-1.00) (39). 'The authors conclude that the presence of endometriosis (pelvic, ovarian, deeply infiltrating endometriosis) on TVUS could establish the diagnosis with high certainty, whereas the absence of radiological evidence of the disease could not confirm that participants are disease free (39).
The typical ultrasound features of endometriomas were assessed in the large patient cohort of the International Ovarian Tumor Analysis (IOTA) studies (51). Based on these characteristics, the following diagnostic rule for an endometrioma was developed: an ovarian cyst with ground-glass echogenicity of the cyst fluid, one to four loc- ules, and no solid parts (51). This diagnostic rule has a sensitivity of 61.4% (95% CI 57.8-64.9), a specificity of 98.3% (95% CI 97.798.7), and a positive predictive value of 90.1% (95% CI 87.1-92.5) (51). It is important to take into account that an endometrioma is only rarely an isolated finding since patients with an endometrioma often have other endometriotic lesions (53). Therefore the diagnosis of an endometrioma should always evoke a detailed investigation for other (peritoneal and deep) endometriotic lesions (2).
The role of TVUS in the diagnosis of deep endometriosis is more complex, given the multitude of possible locations of deep endometriosis. The ESHRE guideline recommends the use of TVUS for identifying or ruling out rectal endometriosis (2).
Data on the accuracy of TVUS for diagnosing other bowel endometriosis lesions are more limited but small individual studies displayed similar performance to that demonstrated for rectosigmoid endometriosis (39).Previously, most of the research on the role of TVUS in deep endometriosis was concentrated on defining the diagnostic sensitivity and specificity of TVUS (54). In recent years, however, the focus has shifted to modified TVUS techniques, which differ from standard TVUS by the introduction of a contrast medium into the vagina or rectum, by preparation of the bowel before the examination or by searching for a landmark linked to the movement of the probe (sliding sign) (39, 54). These new promising techniques have been shown to perform well in a research context, but are also strongly dependent on the operator, with poor repeatability and high interoperator variability when tested in a more routine clinical practice setting (54).
Magnetic resonance imaging
Due to the high costs and limited availability, MRI is not considered as a first-line imaging modality in the diagnosis of endometriosis. However, a growing number of studies suggest that it has a role in the diagnosis of endometriosis because of a greater ability to detect small lesions (55, 56). However, peritoneal endometriotic lesions are only identified by MRI if they are haemorrhagic, greater than 5 mm, or when associated with extensive adhesions distorting the normal anatomy (39).
Since MRI appears to be less accurate for the diagnosis of peritoneal disease, it cannot replace surgery for the diagnosis of endometriosis in general. MRI has a good sensitivity and specificity for the diagnosis of deep endometriosis and endometriomas; however, the added value in addition to TVUS is limited (39). MRI could be useful in the population for whom the risk/benefit ratio of surgery is still unclear (39). The ACOG currently advises MRI, not in routine setting, but only for those with inconclusive ultrasound findings, with high suspicion for rectovaginal or bladder endometriosis (50).
Laparoscopy
Laparoscopic visualization with histological confirmation remains the gold standard for the definite diagnosis of endometriosis (2, 38). A negative diagnostic laparoscopy is highly reliable for the exclusion of endometriosis; however, a positive diagnostic laparoscopy without histological confirmation is inaccurate (57). Data on complication rates of diagnostic laparoscopy for endometriosis are limited. In a systematic review on diagnostic laparoscopy for endometriosis, no direct major complications were reported in any of the included studies, suggesting that laparoscopy is a safe diagnostic intervention, although reporting bias is likely (57).
During laparoscopy, one should systematically evaluate the abdominal cavity, as well as the pelvic cavity for the presence of endometriotic lesions. A good-quality laparoscopy should include systematic checking of (a) the uterus and adnexa; (b) the peritoneum of ovarian fossae, vesicouterine fold, Douglas, and pararectal spaces; (c) the rectum and sigmoid (isolated sigmoid nodules); (d) the appendix and caecum; and (e) the diaphragm. There should also be a speculum examination and palpation of the vagina and cervix under laparoscopic control, to check for ‘buried’ nodules. A good-quality laparoscopy can only be performed by using at least one secondary port for a suitable grasper to clear the pelvis of obstruction from bowel loops, or fluid suction to ensure the whole pouch of Douglas is inspected (2). When ovarian disease is found, the surgeon should be attentive to deep infiltrating, extensive pelvic, and intestinal diseases. Only 1% of all patients with endometriosis of the ovary have solitary lesions restricted to the ovaries (53). All macroscopic findings may be complicated with signs of retraction, pigmentation, and adhesions to the surrounding peritoneum. A histological confirmation is necessary for the diagnosis of endometriosis, since lesions reported as ‘typical’ by the surgeon can be microscopically negative in up to 24% of the cases (58).
Women suffering from chronic pelvic pain, dysmenorrhea, and dyspareunia with a high suspicion of endometriosis are often prescribed hormonal medication and analgesics without a prior definitive laparoscopic diagnosis. It is common practice for laparoscopy to be performed if the patient does not react favourably to the prescribed medical or hormonal treatment. In a retrospective study, relief of chronic pelvic pain symptoms, or lack of response, with preoperative hormonal therapy was not an accurate predictor of the presence or absence of histologically confirmed endometriosis at laparoscopy (59). Furthermore, empirical treatment can lead to a delay in diagnosis associated with significant social and psychological disadvantages (59). The ESHRE 2014 guideline recommends to rule out other causes of pelvic pain as far as possible and thoroughly counsel patients with presumed endometriosis before starting empirical treatment (2).
More on the topic Phenotypes and staging of endometriosis:
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Introduction