Placental-related disorders of pregnancy
Placental-related disorders of pregnancy are almost unique to the human species. These disorders, which affect around a third of human pregnancies, primarily include miscarriages, pre-eclampsia, and FGR.
In other mammalian species, the incidence of these disorders is extremely low. In humans, these disorders may relate to the fact that our invasive form of implantation, and subsequent haemochorial placentation, poses special haemodynamic challenges. These complications are often associated with abnormal maternal adaptations to pregnancy in the second trimester, including failure to gain weight, lack of blood pressure reduction, and persistent non-pregnant haematocrit levels (17).There is mounting evidence that once organogenesis is complete, oxidative stress plays a major role in both the physiological changes associated with the remodelling of the human placenta and the pathophysiology of placental-related disorders of pregnancy (8, 41). Pathological oxidative stress arises when the production of reactive oxygen species overwhelms the intrinsic antioxidant defences, causing indiscriminate damage to biological molecules and leading to loss of function and cell death.
Miscarriages
First-trimester pregnancy losses are the consequence of an extreme disorder of placentation with rapid degeneration of the placental tissue, independently of the aetiology (8). In about two-thirds of first-trimester miscarriages there is anatomical evidence of defective placentation, which is mainly characterized by a thinner and fragmented trophoblastic shell, reduced cytotrophoblast invasion of the endometrium, and incomplete plugging of the lumen at the tips of the spiral arteries (42, 43). These deficiencies are associated with the absence of physiological changes in most of the spiral arteries, and lead to premature and disorganized onset of the maternal circulation throughout the entire placenta (Figure 9.7).
Independent of the cause of the miscarriage, the excessive entry of maternal blood into the intervillous space has two effects; a direct mechanical effect on the villous tissue, which becomes progressively enmeshed inside large intervillous blood thrombi, and widespread indirect oxygen-mediated trophoblastic oxidative damage, with increased apoptosis (44, 45). Overall, the consequences are placental degeneration with extensive loss of syncytiotrophoblast function and detachment of the placenta from the uterine wall. This mechanism is common to all miscarriages with the time at which it occurs dependent on the aetiology, aneuploidies being associated with early (5-9 weeks) and maternal antiphospholipid syndrome with late (1014 weeks) placental degeneration (41).
Pre-eclampsia
There is increasing evidence that pre-eclampsia is a heterogeneous syndrome, and early- and late-onset forms are now recognized with a distinction of onset before or after 34 weeks of gestation (46). Early-onset pre- eclampsia stems from a similar, though lesser, defect in early trophoblast invasion as in spontaneous miscarriage, whereas
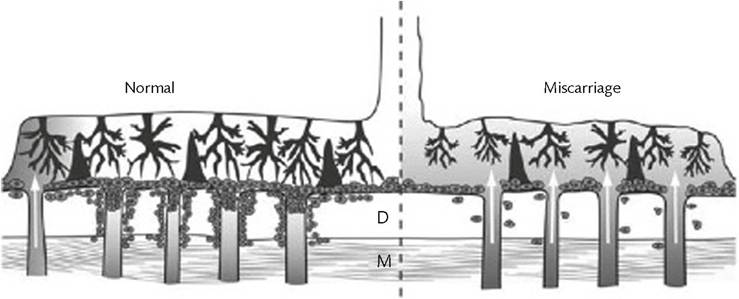
Figure 9.7 Diagrammatic representation of the trophoblast invasion in a normal pregnancy and a miscarriage. In miscarriages, the shallow invasion of the deciduas (D) and superficial myometrium (M) results in a deficient plugging of the spiral arteries and early onset of the intervillous circulation.
late-onset pre-eclampsia is thought to reflect maternal predisposition to cardiovascular disease.
In early-onset pre-eclampsia, while invasion is sufficient to anchor the gestational sac it is too shallow for complete transformation of the spiral arteries into low-resistance channels (47). As a consequence, the spiral arteries retain smooth muscle cells within their walls, particularly in their myometrial segments (Figures 9.2 and 9.3), and remain responsive to circulating vasoactive compounds.
This may lead not only to diminished perfusion of the intervillous space, but more importantly to intermittent perfusion. Since the placenta and fetus continually extract oxygen it is expected that transient hypoxia will result, and that consequently the placenta suffers a chronic low-grade ischaemia-reperfusion type injury (48). By contrast to miscarriage where there is rapid and generalized degeneration of the placental tissue, in pre-eclampsia the damage is progressive and can be compensated for some time depending on the severity of the deficiency in both spiral arterial remodelling and placental intrinsic antioxidant capacity.For many years, pre-eclampsia has been considered to be a two-stage disease. Pre-eclampsia is at least a three-stage disorder starting with the primary pathology being an excessive or atypical maternal immune response leading to insufficient placentation (8, 49). Dysfunctional perfusion of the intervillous space of the placenta leads to oxidative and haemodynamic stress. Chronic trophoblastic oxidative stress releases excessive proinflammatory and antiangiogenic factors into the maternal circulation leading to diffuse maternal endothelial cell dysfunction and the clinical symptoms of pre-eclampsia. Early-onset pre-eclampsia is therefore predictable from the beginning of the second trimester because of the major syncytiotrophoblast stress in early pregnancy and the corresponding changes in its biomarkers (50). By contrast, prediction of late-onset pre-eclampsia is poor because there is no early trophoblast pathology in these cases.
Placental insufficiency and fetal growth
FGR is a failure of the fetus to reach its full growth potential. The definition is conceptual but impossible to verify, because it is not possible to determine the exact growth potential of an individual fetus. In practice, smallness, with or without evidence of fetal response to undernutrition, is used to ascertain FGR. It can have many causes, but the majority of cases that have no genetic or infectious aetiology are thought to arise from abnormal placentation.
Pathological studies have demonstrated deficient physiological conversion of the arteries as in pre-eclampsia, but to a lesser degree, especially in the myometrial segment and a positive correlation between the birth weight and the degree of conversion (51).The distinction between ‘placental’ and ‘maternal’ causation has been proposed, with ‘placental’ cases being more frequently associated with early-onset pre-eclampsia and FGR (52). In cases of isolated FGR, there is scanty evidence showing the level of stress is either similar to the normal control or intermediate between a normal control and an early-onset pre-eclamptic placenta. The fact there is morphological and molecular evidence of oxidative stress in most FGR placentas indicates a chronic low-level oxidative stress may occur from the time of onset of the maternal circulation onwards, and leads to a lower growth trajectory of the placenta. This is consistent with the reduced rate of growth of the placenta observed with serial ultrasound scans in these cases (50).