Prenatal screening, diagnosis, and management of common placental and cord anomalies
Before the development of ultrasound imaging, morphological examination of the placenta and the cord was only of epidemiological value and was therefore of little influence on pregnancy management.
With modern ultrasound equipment, it is now possible to examine the placenta and the cord in detail from the beginning of the first trimester and screen for placental and umbilical cord structural anomalies that are associated with perinatal complications (53-61).Anomalies of placentation
Placenta praevia is defined as implantation of the placenta fully or partially in the lower uterine segment. Determining placental location was the first aim of placental routine examination in vivo. Placenta praevia has a prevalence of 4-5 per 1000 pregnancies and is associated potentially with life-threatening complications for the mother, including severe ante- and postpartum bleeding, need for hysterectomy, blood transfusions, septicaemia, and thrombophlebitis, and adverse fetal and neonatal outcome including preterm
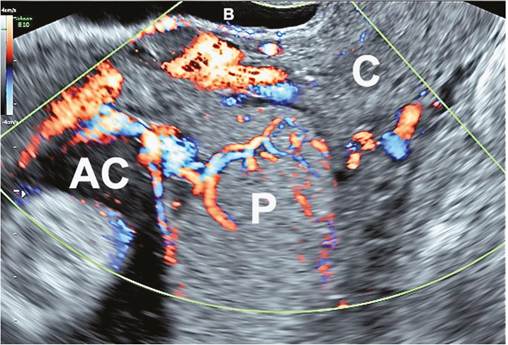
Figure 9.8 Transvaginal ultrasound image of the cervix (C) and placenta (P) at 32 weeks of gestation showing a major placenta praevia covering the cervix (grade IV). AC, amniotic cavity; B, bladder.
delivery and perinatal death (53). Placenta praevia is more common in multiple gestation pregnancy and in pregnancies following a caesarean section delivery (53, 54).
Placental location is usually reported during the routine anomaly scan at 20-22 weeks of gestation. If the placenta is found to be reaching, overlapping, or covering the internal cervical os, a followup scan should be scheduled at the beginning of the third trimester (28-30 weeks) before the lower uterine segment starts to form. Almost 90% of the placentas defined as low around mid gestation are found to be completely outside of the lower uterine segment later in gestation, and are entirely safe (53).
Transvaginal ultrasound is the preferred technique for assessment of placental location, particularly in suspected low posterior placentas. The term ‘placenta praevia' should only be used when the placental edge covers, overlaps, or is within 2 cm of the internal cervical os in the third trimester. If the placental edge is located further than 2 cm but within 3.5 cm from the internal cervical os, the placenta should be termed low lying. In the latter case, there is a good chance of a vaginal delivery but the incidence of postpartum haemorrhage remains high.A placenta that covers the entire internal cervical os is classified as major placenta praevia (Figure 9.8) and always requires a caesarean delivery. Caesarean section for major placenta praevia is associated with a high risk of massive intra- and postpartum bleeding which will require blood transfusion and possible admission of the mother to intensive care. Additional surgical procedures including hysterectomy may be required in case of excessive bleeding during delivery, and thus caesarean sections for major placenta praevia should be planned to occur in a tertiary care centre with management by a multidisciplinary team.
Placenta accreta spectrum (PAS) is defined as an abnormally adherent or invasive placenta to the uterine wall (53). When the villi invade deeply into the myometrium it is described as increta and when the villi penetrate the entire thickness of the uterine wall and beyond it is reported as percreta. The vast majority of PAS are found in women with placenta praevia and also a previous caesarean section. Recent epidemiological studies have also found that the strongest risk factor for placenta praevia is a prior caesarean section suggesting that a failure of decidualization in the area of a previous uterine scar can have an impact on both implantation and placentation (55, 56). PAS cases have an overall maternal and fetal mortality rate of around 10% each, due to massive intrapartum or postpartum bleeding (53-58).
Attempts to remove an undiagnosed PAS may provoke further bleeding and a cascade of ongoing haemorrhage, shock, and coagulation disorders requiring complex clinical management. Thus prenatal diagnosis of this condition is pivotal to allow the surgical team to demarcate the areas of the placenta that require resection before surgery and/or to consent the patient for additional procedures such as a caesarean hysterectomy.The most common sonographic finding associated with PAS is the enlargement of the underlying uterine vasculature with the presence of intraplacental lacunae (55). The addition of colour or power Doppler evaluation has been valuable in improving the diagnosis of of invasive PAS (55, 56). All women presenting with a history of previous caesarean delivery or uterine surgery and an anteriorly situated low-lying or placenta praevia at the anomaly scan require a detailed examination of the placenta and follow-up scan at 28 weeks for the identification of PAS (53). Women managed by a multidisciplinary care team are less likely to require large-volume blood transfusion, reoperation within 7 days of delivery for bleeding complications, and to experience prolonged maternal admission to the intensive care unit, large-volume blood transfusion, coagulopathy, and urethral injury than women managed by standard obstetric care (53, 58).
Vascular anomalies of the placenta
Thrombosis and infarcts are usually found during the third trimester of pregnancy and are often associated with placental-related disorders of placentation (51, 62). Placental thromboses are the result of focal coagulation of blood in the intervillous space and appear on ultrasound examination as large hypoechoic central areas of turbulent blood flow surrounded by an echogenic shell of villi embedded in fibrin. Extensive infarcts are found in pregnancies complicated by pre-eclampsia or essential hypertension, and are associated with an increase in perinatal mortality and intrauterine growth retardation. Sonographically, placental infarcts appear as large intraplacental areas, irregular and hyperechoic in the acute stage and isoechoic in a more advanced stage.
In pre-eclampsia with FGR, infarcts are often associated with microscopic diffuse villitis and excessive fibrin deposition (51), which is probably secondary to major impairment of the uteroplacental circulation. These placental vascular lesions are more frequent in twins, and pre-eclampsia is associated with a higher incidence of placental infarctions and thrombosis in dichorionic twin placentas than in monochorionic twins and singletons (54).Haematomas are the results of extravasation of maternal or fetal blood and may be subamniotic, subchorionic, or retroplacental (63, 64). A subchorionic or retroplacental haematoma reflects bleeding of maternal origin and is identified sonographically as a hypoechoic area between the chorion and uterine wall (Figure 9.9). Such lesions are seen in more than 1% of pregnancies, commonly in the first trimester. In very early pregnancy (at delivery of 0.5-1% of placentas examined (70). Chorioangiomas are non-trophoblastic tumours of the placenta derived from excessive vascular proliferation within the stroma of chronic villi. The incidence of large chorioangiomas is lower and varies from 1 in 8000 to 1 in 50,000 pregnancies. These tumours are well circumscribed, have a different echogenicity from the rest of the placental tissue, and have often been documented sonographically from 16 weeks of gestation. Chorioangiomas can be complicated by fetal hydrops due to congestive heart failure and secondary to chronic shunting of large volumes of fetal blood through the tumour (70). Polyhydramnios is also a common complication of chorioangiomas and like hydrops is linked to its vascular nature of the tumour and not to size. Abnormal cardiovascular profile scores have recently been observed in 46% of chorioangiomas, and 39% of those cases show a poor neurodevelopmental outcome after birth (71). The fetal risk depends on the proportion of angiomatous versus mixoid tissue inside the chorioangioma, and thus prenatal identification of the vascularization of the tumour with colour Doppler imaging is essential for the management of this tumour.
If the tumour is avascular, no specific complications should be expected (70). If the tumour is vascularized, and in particular if it contains numerous large vessels, serial ultrasound and Doppler examinations are warranted to detect polyhydramnios and fetal cardiovascular dysfunction.Anomalies of the umbilical cord
A single umbilical artery (SUA) cord is the result of the absence of one of the two normal arteries, and is one of the most common congenital fetal malformations with an incidence of approximately 1% of all deliveries (72). SUA occurs three to four times more frequently in twins, and almost invariably accompanies the acardia malformation and sirenomelia or caudal regression syndrome (54, 72). There is also a sixfold increase of the incidence of marginal and velamentous insertion of the cord among SUA infants. Major fetal anatomical defects are largely responsible for the high fetal and neonatal loss from this pathology and can affect any organ system. The discovery of a SUA in the perinatal period justifies a detailed ultrasound examination of the neonate to exclude minor anomalies of internal organs, such as the kidney or heart. The incidence of FGR is significantly elevated among fetuses with a SUA and may be present without any other congenital anomalies in 15-20% of the cases (72). SUA twins are at higher risks of FGR and preterm delivery. Discordance for SUA in monochorionic twins can be present, and provides evidence against an exclusively genetic origin of this anomaly (54).
Vasa praevia are fetal vessels running through the membranes, over the cervix, and under the fetal presenting part, unprotected by the placental tissue or the umbilical cord (59, 60). This particular vascular arrangement is usually the result of a velamentous insertion of the umbilical cord in a single or bi-lobed placenta (vasa praevia type 1) or the presence of aberrant fetal vessels running between one or more accessory lobes of the placenta (vasa praevia type 2).
Velamentous insertion of the cord (VCI) is a well-defined pathological entity with a frequency around 1% of pregnancies (55, 56). Approximately 90% of women with vasa praevia have VCI and 3- 4% of women with a VCI have vasa praevia. VCI of one of the umbilical cords is eight times more common in twins than in singletons. Monochorionicity doubles the risk for VCI. The incidence of VCI, vasa praevia, or marginal cord insertion is higher in assisted reproductive technology than in spontaneously conceived singletons, but is similar in both types of twins (73, 74).Vasa praevia is more common in women in whom the placenta was low lying in the mid pregnancy, but appears to migrate with advancing gestation.
In vasa praevia, vessels are vulnerable to compression changes since they are not supported by Wharton's jelly, and when the cervix is dilated and the rupture of the membranes occurs these unprotected vessels are at risk of rupture and fatal fetal haemorrhage. The classic presentation of undiagnosed vasa praevia in labour is the presence of painless vaginal bleeding usually after the rupture of the membranes associated with acute fetal distress evidenced by CTG changes or fetal demise. The absence of a normal insertion of the umbilical cord in the placenta, VCI, can be reliably detected by the use of colour Doppler ultrasound (Figure 9.10). Thus women with VCI, multiple pregnancies, bi-lobated placenta, and placenta praevia should be screened for vasa praevia (59, 60).