Postpartum haemorrhage
The incidence of maternal death from obstetric haemorrhage in the United Kingdom is 0.55 per 100,O0O maternities (1). Substandard care is regularly identified in reviews of maternal deaths from haemorrhage: specifically, a lack of routine postpartum monitoring, a failure to act on the signs and symptoms of a deteriorating woman, and a lack of early senior multiprofessional involvement (15).
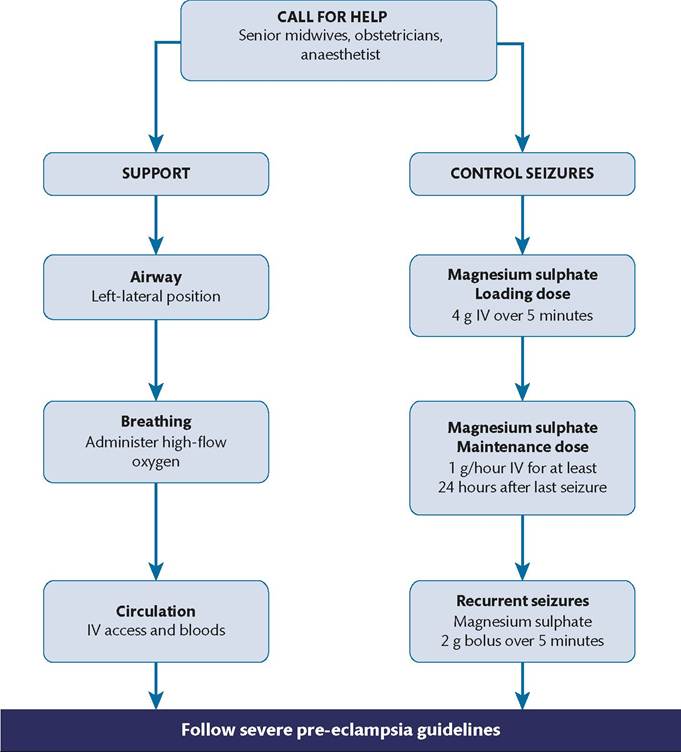
Figure 29.5 Algorithm for the initial management of eclampsia.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi-Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.
Primary postpartum haemorrhage (PPH) is traditionally defined as blood loss of 500 mL or more within the first 24 hours after birth. Major PPH is categorized as blood loss of greater than 1000 mL, and can be divided into moderate PPH (1000-2000 mL) and severe PPH (>2000 mL) (18).
Primary PPH is usually caused by at least one of what are often classified as the ‘the four Ts':
• Tone (e.g. uterine atony)
• Tissue (e.g. retained membranes or placenta)
• Trauma (e.g. tears of the genital tract)
• Thrombin (e.g. coagulopathies).
Secondary PPH is a blood loss of 500 mL or more from 24 hours after birth until 12 weeks postpartum. The most common cause is endometritis, which usually responds to antibiotic treatment and removal of any retained products of conception.
Immediate management of a major PPH
Key tips to enable effective management:
• Prompt recognition.
• Call for help.
• Uterine massage or bimanual compression (the most likely cause of a primary PPH is an atonic uterus).
• Fluid resuscitation.
• Administer uterotonics if appropriate.
• Restore blood volume and oxygen-carrying capacity.
• Replace blood products early.
• Low threshold for transfer to theatre.
• Early recourse to hysterectomy.
PPH is usually overt due to vaginal bleeding. However, bleeding can be concealed (e.g. broad ligament haematoma). The only indication may be a deterioration of postpartum observations or the woman exhibiting signs of shock. It is important to closely monitor the postpartum woman, ideally documenting observations on a MOEWS chart and promptly acting upon any concerning features.
An algorithm for the initial management of a major PPH is displayed in Figure 29.7.
Figure 29.6 An eclampsia emergency box.
Activate the emergency buzzer to call for urgent help from the multiprofessional team: senior midwives, obstetricians, and anaesthetists. State the problem clearly: ‘This is a postpartum haemorrhage’. Request the PPH emergency box; an example is shown in Figure 29.8. Consider activation of the code red major obstetric haemorrhage protocol.
Each maternity unit should have a major obstetric haemorrhage protocol with agreed criteria for activation. This will usually alert additional team members and initiate the preparation of blood products. The blood transfusion laboratory technicians, porters, and consultant clinical haematologist must be informed and on standby should urgent blood products be required. The theatre team should prepare the operating theatre for possible urgent transfer. The consultant obstetrician and anaesthetist should be informed early in cases of major PPH with ongoing blood loss.
Initial actions
•Lie the woman flat.
•Administer high-flow oxygen.
•Massage the uterus to rub up a contraction and expel any clots.
•Assess ABC.
•Obtain intravenous access with two large-gauge cannulae.
• Send bloods for full blood count, urea and electrolytes, and clotting screen including fibrinogen and crossmatch 4 units of blood.
• Rapid fluid resuscitation with at least 2 L of Hartmann’s solution.
Restoration of the blood volume and oxygen-carrying capacity is vital for aiding resuscitation. Up to 3.5 L of fluid can be infused: 2 L of crystalloid as rapidly as possible, followed by up to 1.5 L of colloid if blood is not available. Intravenous fluids should be warmed, as the woman can become cold due to the massive transfusion, further exacerbating the risk of disseminated intravascular coagulation.
Blood products should be replaced early. The woman’s clinical picture will determine whether blood products are required, rather than awaiting laboratory blood results. If cell salvage is available, this should be set-up and commenced. If cell salvage is not possible, crossmatched blood is preferable. O rhesus-negative blood or noncrossmatched group-specific blood can be given if crossmatched blood is not available. Additional blood products such as fresh frozen plasma and cryoprecipitate may be indicated at a later stage; obtain advice from the haematologist and consultant anaesthetist.
During the management of the PPH, constantly re-evaluate the condition of the woman, her response to treatment, and the estimated blood loss. Point-of-care testing, such as ROTEM, can be used for a quick assessment of coagulation. Monitor blood pressure, heart rate, respiratory rate, and pulse oximetry continuously if possible. Document observations, including temperature and fluid input and output, on a high-dependency chart. Assign a scribe to document all timings and actions.
Stop the bleeding
• Investigate the cause of the bleeding:
■ Check the uterine tone and height of the fundus.
■ Massage the uterus to expel any clots.
■ Examine for tears of the vagina, cervix, or perineum.
■ Ensure the placenta has delivered and check it is complete.
■ Examine the woman for signs of clotting disorders, such as bleeding from wound or cannula sites.
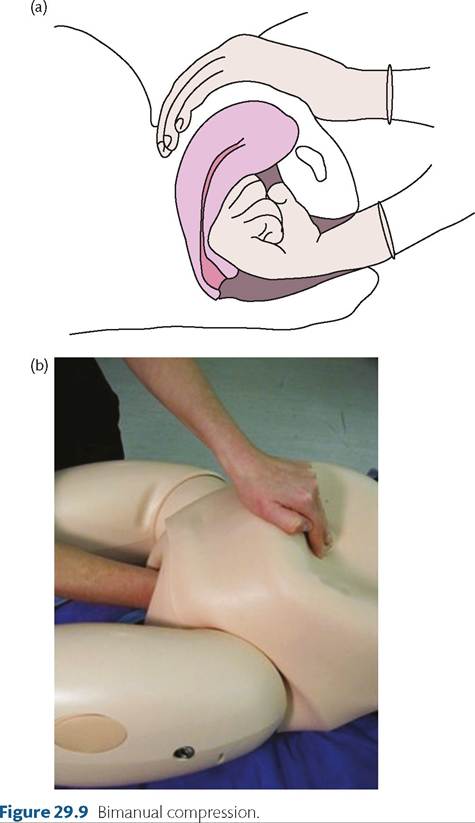
• Perform bimanual compression if the uterus is atonic: uterine atony is the most common cause of PPH. Bimanual compression, as demonstrated in Figure 29.9, encourages contraction of the uterus and is especially useful as a holding measure if travelling in an ambulance or awaiting transfer to the labour ward or theatre.
■ How to perform bimanual compression: gently insert one hand into the vagina and form a fist. Apply pressure against the anterior wall of the uterus. With the other hand on the abdomen, press on the uterine fundus and compress the uterus between both hands. Continue bimanual compression until the uterus contracts.
• Administer oxytocic medication: active management of the third stage of labour is recommended for all women (19). First- line medication is 10 mg Syntocinon (oxytocin) or 1 ampoule of Syntometrine (oxytocin plus ergometrine), both administered intramuscularly. If the woman has not received any oxytocics, administer one dose. If the woman has already had an oxytocic, a second dose can be given.
■ The blood pressure must always be checked prior to giving Syntocinon or Syntometrine. Syntocinon boluses should be used with caution in women with severe hypotension, as the blood pressure may drop further (11). Ergometrine can cause hypertension, therefore Syntometrine is contraindicated in women with high blood pressure.
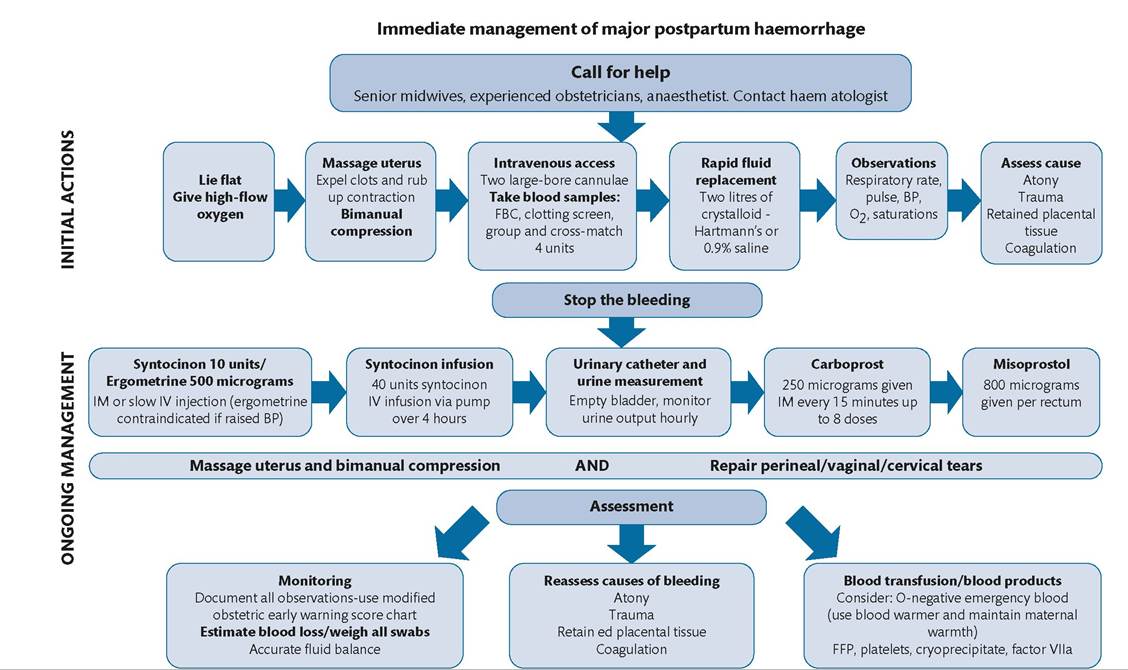
Figure 29.7 Algorithm for the initial management of a major postpartum haemorrhage.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi-Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.
■ If the uterus contracts following the oxytocics, consider commencing a Syntocinon infusion (oxytocin 40 units in 500 mL physiological saline infused via a pump at 125 mL/hour over 4 hours) to maintain uterine tone. However, this will not initiate uterine tone, therefore additional measures will be required if the uterus has not contracted.
Figure 29.8 A PPH emergency box.
• Catheterize the bladder: a full bladder may inhibit contraction of the uterus. Insert an indwelling Foley catheter to ensure the bladder is empty and enable monitoring of urine output.
• Repair any tears: bleeding from tears is the second most common cause of PPH. If the tear is easily visible in the labour room and analgesia is adequate, repair the tears as soon as possible.
• Transfer to theatre: have a low threshold for transfer to theatre for examination under anaesthesia, particularly in cases of ongoing bleeding, if you suspect retained products of conception or if tears are not easily accessible.
■ The method of anaesthesia (general or regional) should be discussed between the anaesthetist, obstetrician, senior midwife, and the woman (if appropriate).
• Examination under anaesthesia: feel within the uterus to ensure it is empty and systematically inspect the genital tract to identify any tears.
■ Most cases of major haemorrhage will have settled after these measures. If the bleeding is ongoing, consider alternative medications, mechanical and surgical measures.
• Uterotonic medications: if the uterus is still atonic, give carboprost (Haemabate) 250 mcg intramuscularly every 15 minutes up to a maximum of eight doses. Carboprost is a prostaglandin analogue. Side effects include diarrhoea, vomiting, hypertension, headache, and bronchospasm. Carboprost is contraindicated in women with cardiovascular or respiratory disease, including asthma.
■ Misoprostol is a less effective, inexpensive prostaglandin analogue; 800-1000 mcg per rectum can be administered if other uterotonics are not available or contraindicated.
• Tranexamic acid: tranexamic acid is an antifibrinolytic that is used for prophylaxis and treatment of haemorrhage in many other specialties, including orthopaedics and emergency medicine—1 g of tranexamic acid intravenously is thought to reduce PPH in obstetric patients.
■ A systematic review concluded that prophylactic tranexamic acid in conjunction with uterotonics decreased postpartum blood loss after vaginal birth and caesarean section (20). However, these studies were of varying quality and were not large enough to assess the effect on maternal outcomes. Most recently, the World Maternal Antifibrinolytic (WOMAN) trial, an international randomized controlled trial, recruited over 20,000 women with clinically diagnosed PPH to receive tranex- amic acid or placebo. When tranexamic acid was given alongside uterotonics as soon as possible after the onset of primary PPH, the trial demonstrated a significant reduction in maternal deaths from haemorrhage following vaginal and caesarean birth and a reduction in the number of women requiring laparotomy to control bleeding. There was no increase in vascular occlusive events.
■ A reasonable and safe option for the management of PPH is 1 g of tranexamic acid intravenously and this can be repeated after 30 minutes.
• Mechanical and surgical measures: intrauterine balloons, such as Rusch or Bakri balloons, are often an effective measure to tamponade the uterus. Insert the balloon catheter into the uterus and inflate with 250-500 mL of warmed saline. If the bleeding settles, leave the balloon in place for up to 24 hours.
• Additional measures: these include insertion of a B-lynch suture, interventional radiology, ligation of the internal iliac artery, and hysterectomy. There should be early recourse to hysterectomy in cases of life-threatening unrelenting haemorrhage, before the woman is severely compromised or develops disseminated intravascular coagulation. Ideally a second opinion should be sought from a senior doctor; but this should not unduly delay hysterectomy in life-threatening situations.