Acute uterine inversion
Acute uterine inversion is a rare occurrence, affecting anywhere from 1:1500 to 1:20,000 births (22, 23). The uterus turns ‘inside out', with the fundus descending through the genital tract:
• Grade I: the fundus inverts down to the cervical canal.
• Grade 2: the fundus inverts into the vagina.
• Grade 3: the fundus is visible at/outside of the introitus.
Acute uterine inversion most commonly results from early or excessive traction on the umbilical cord. Additional risk factors include fundal pressure, short umbilical cord, adherent placenta, previous caesarean section, manual removal of placenta, abnormalities of the uterus (e.g. unicornuate uterus), connective tissue disorders (e.g. Ehlers-Danlos syndrome), multiparity, previous uterine inversion, precipitate labour, and fetal macrosomia.
Diagnosis of acute uterine inversion
The diagnosis may not be obvious as the uterus may not be visible outside of the introitus and vaginal blood loss is often minimal initially. Most commonly, the woman develops presyncopal symptoms that then progress into signs of neurogenic shock. As the uterus inverts through the cervix, vagal stimulation results in maternal bradycardia and hypotension. The uterus may not be palpable on abdominal examination. Vaginal examination will often reveal a mass in the vagina, which is the uterus. Atonic PPH ensues in 90% of cases (24, 25), usually once the uterus has been replaced and the placenta has been removed. The woman is likely to develop hypovolaemic shock.
Immediate management of acute uterine inversion
An algorithm for the immediate management of acute uterine inversion is displayed in Figure 29.10.
Replacement of the uterus is more likely to be successful if attempted early. As time progresses, the uterus will become oedema- tous and may develop constriction rings. Uterine relaxation may be useful in these cases but should be used with caution, as they
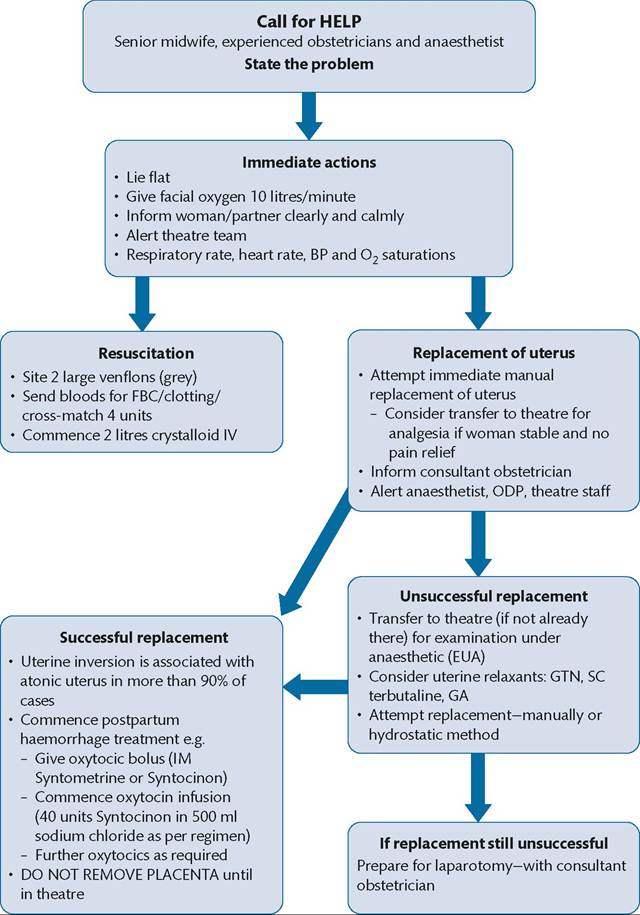
Figure 29.10 Algorithm for immediate management of acute uterine inversion.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi-Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.
may conversely exacerbate atonic PPH. Uterine relaxation can be achieved with tocolytics, for example, terbutaline 250 mcg subcutaneously or glyceryl trinitrate spray. General anaesthesia may also relax the uterus.
There should be a low threshold for transfer to theatre. If the woman is bleeding, IS haemodynamically unstable, or has effective analgesia, attempt to manually replace the uterus immediately, wherever the woman is situated. However, if the woman is stable, does not have adequate analgesia, or if initial attempts at manual replacement are unsuccessful, transfer to theatre is advisable. The method of anaesthesia should be chosen according to the woman's clinical status. Once the uterus has been replaced, administer oxytocics to enable uterine contraction and reduce the risk of PPH.
Replacement of the uterus
If the placenta is still in situ, do not attempt to remove it until the uterus is replaced. Prophylactic intravenous antibiotics should be administered as per local guidelines.
• Manual replacement: put a hand into the vagina and follow the umbilical cord up to the fundus of the uterus. Gently raise the fundus towards the abdominal cavity with your hand until it reverts into its anatomical position. Leave your hand in position holding the uterus for a few minutes afterwards, to ensure the position is maintained and to encourage uterine contraction.
• Hydrostatic method: hydrostatic pressure is achieved by sealing the introitus with a hand or a silastic ventouse cup and inserting fluid into the vagina under pressure. This distends the vagina and facilitates replacement of the uterus, usually within 10 minutes. Prior to this procedure, it is important to check that there are no large vaginal lacerations.
Place the silastic ventouse cup into the vagina, creating a seal. Rapidly infuse 2 L of slightly warmed normal saline into the vagina, via a blood giving set attached to the end of the silastic ven- touse cup. Inflate a pressure jacket or raise the fluid bag at least 1 metre above the level of the vagina to provide enough pressure for insufflation of the vagina.
• Surgical management: it is rare for the previously listed methods to not be successful. Laparotomy may be required in difficult cases. Huntington’s operation, upward traction on the uterus from the abdominal cavity, is first-line surgical management. If this is not successful, Haultain’s operation involves vertical incision of the cervical ring posteriorly to aid replacement.