Umbilical cord prolapse
Umbilical cord prolapse is defined as the descent of the umbilical cord through the cervix alongside (occult) or past (overt) the presenting part in the presence of ruptured membranes (26).
This commonly occurs after the amniotic membranes rupture and when the fetal presenting part is poorly applied to the maternal cervix. Cord prolapse causes cord compression and vasospasm of the umbilical arteries, which reduces blood flow to and from the fetus, resulting in birth asphyxia. Earliest possible birth is crucial to improving outcomes (26).Cord prolapse occurs in 0.1-0.6% of all births. In breech presentations, the incidence is 1%. The associated perinatal mortality rate is approximately 9% (27). This is most commonly due to complications of prematurity and congenital anomalies, which are predisposing factors for cord prolapse, rather than intrapartum asphyxia.
Risk factors for cord prolapse
Antenatal
• Breech presentation
• Unstable, oblique, or transverse lie
• Polyhydramnios
• Congenital anomalies
• External cephalic version
• Expectant management of premature rupture of membranes
• Previous cord prolapse.
Intrapartum
• Amniotomy (especially with a high presenting part)
• Prematurity
• Breech presentation
• Internal podalic version
• Second twin
• Disimpaction of fetal head during rotational operative vaginal birth
• Fetal scalp electrode application.
Management of cord prolapse
Figure 29.11 demonstrates the mnemonic ‘CORD’, which outlines the key steps in management of cord prolapse: Consider, Organize help, Relieve pressure, and Decision for birth (26).
Consider
A prolapsed cord may be seen outside of the vagina, but this is uncommon. Suspect cord prolapse when there is an abnormal fetal heart rate pattern, particularly if the membranes have recently ruptured. Cord prolapse should also be considered when there are associated risk factors.
Approximately half of the reported cases of cord prolapse are iatrogenic, such as membrane rupture with a high presenting part. A speculum examination or vaginal examination should be performed to exclude cord prolapse in these cases.Organize help
Activate the emergency bell to call for urgent help from the multiprofessional team: senior midwives, senior obstetricians, anaesthetists, theatre staff, and the neonatal team. State the problem clearly: ‘This is a cord prolapse’.
If the emergency occurs outside hospital, call an emergency ambulance immediately to transfer the woman to the nearest consultant- led obstetric unit. Contact the obstetric unit directly to inform them of the emergency and the estimated time of arrival, so that preparations can be made to assist the birth as soon as possible after arrival.
If the birth of the baby is imminent, continue to call a paramedic ambulance in case of neonatal compromise requiring urgent neonatal review in hospital.
Relieve pressure
Relieve pressure on the cord by elevating the presenting part and, if applicable, reducing contractions. These measures are useful while preparing for birth; however, birth should not be delayed by trying to implement them.
• Maternal positioning: advise the woman to adopt a knee-chest face-down position while awaiting transfer to theatre or hospital. For ambulance transfer, the exaggerated Sim’s position (left- lateral with a pillow under the left hip) with or without Trendelenburg (tilted bed so that the woman’s head is lower than the pelvis) may be more stable and hence safer.
• Digital elevation: manually elevate the presenting part with two fingers to reduce compression of the cord. If the cord has prolapsed outside of the vagina, gently attempt to replace it into the vagina. Handling of the cord must be kept to a minimum, as this may cause vasospasm. Continue manual elevation during transfer to theatre and the administration of anaesthesia, until immediately prior to birth.
• Bladder filling: alternatively, you can fill the bladder to elevate the presenting part. This is often useful when there is a delay, such as awaiting transfer to hospital.
■ Insert a Foley catheter into the bladder and fill with 500-750 mL of sterile physiological 0.9% saline via a blood giving set. Clamp off the giving set once the bladder is filled and leave attached to the catheter, to ensure the volume is maintained. Disconnect the giving set and empty the bladder immediately
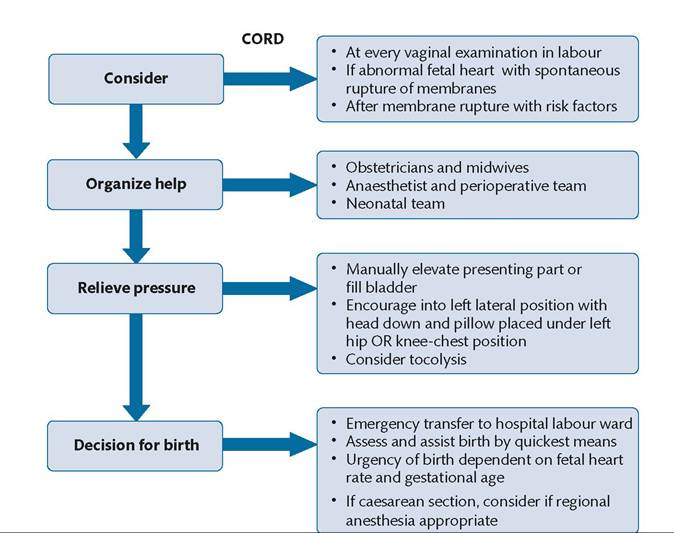
Figure 29.11 'CORD': the key steps for the management of cord prolapse.
Source data from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, editors. PROMPT: PRactical Obstetric Multi-Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012, pp. 169-78.
prior to birth, whether this is by caesarean section or operative vaginal birth.
• Reducing contractions: if an oxytocin infusion is in progress, this should be discontinued. If there are persistent fetal heart rate abnormalities, consider tocolysis with terbutaline 250 mcg subcutaneously. Be prepared for an increased risk of PPH associated with tocolytic administration.
Decision for birth
If the cervix is not fully dilated, perform a caesarean section. The urgency of caesarean section depends on the fetal heart rate pattern and gestational age. If the fetal heart rate pattern is normal, then a category 2 birth may be acceptable. However, you must continually assess the situation and upgrade to category 1 birth if there is any deterioration.
The urgency and timing ofbirth should be discussed between the anaesthetic, obstetric, and midwifery teams, to ensure the safest method of anaesthesia is chosen. If the anaesthetist is attempting regional anaesthesia, continue to reassess the urgency and timing of birth and avoid prolonged and repeated attempts at regional anaesthesia.
If the cervix is fully dilated and you anticipate that vaginal birth is achievable quickly and safely, consider an operative vaginal birth.
Breech extraction can be considered in certain circumstances, such as after internal podalic version for the second twin.