Shoulder dystocia
Shoulder dystocia is diagnosed when routine axial traction fails to complete the birth of the baby after the birth of the head, and additional manoeuvres are required to release the fetal shoulders.
This is usually due to the anterior fetal shoulder impacting upon the maternal symphysis pubis. The posterior fetal shoulder can impact upon the maternal sacral promontory, but this is less common.There is a wide variation in the reported incidence of shoulder dystocia (28). Studies involving the largest number of vaginal births report incidences between 0.58% and 0.70% (29-34). Shoulder dystocia is unpredictable, as the majority of cases occur in women without any risk factors, and it is therefore largely unpreventable. Clinicians should be aware of existing risk factors, but should also be alert to the possibility of shoulder dystocia with any birth (35).
Risk factors for shoulder dystocia
• Prelabour:
■ Previous shoulder dystocia
■ Macrosomia greater than 4.5 kg
■ Maternal diabetes mellitus
■ Maternal obesity
• Intrapartum:
■ Prolonged first stage
■ Prolonged second stage
■ Augmentation of labour
■ Operative vaginal birth.
Recognition of shoulder dystocia
• There may be difficulty with the birth of the face and chin.
• When the head is born, it remains tightly applied to the vulva.
• The chin retracts and depresses the perineum—the ‘turtle-neck’ sign.
• The anterior fetal shoulder fails to release with maternal pushing and routine axial traction.
Routine traction is defined as ‘the traction required to release the fetal shoulders in a vaginal birth where there is no difficulty with the shoulders' (36). Axial traction is traction in line with the fetal spine. Traction should be slow and gentle.
In cases of shoulder dystocia, traction alone will not release the fetal shoulder from behind the symphysis pubis.
Excessive traction, downward traction, and sudden jerking movements must be avoided, as they all increase the risk of brachial plexus injury. Additionally, fundal pressure must not be performed, as this will further impact the shoulder and increase the risk of brachial plexus injury as well as uterine rupture.Management of shoulder dystocia
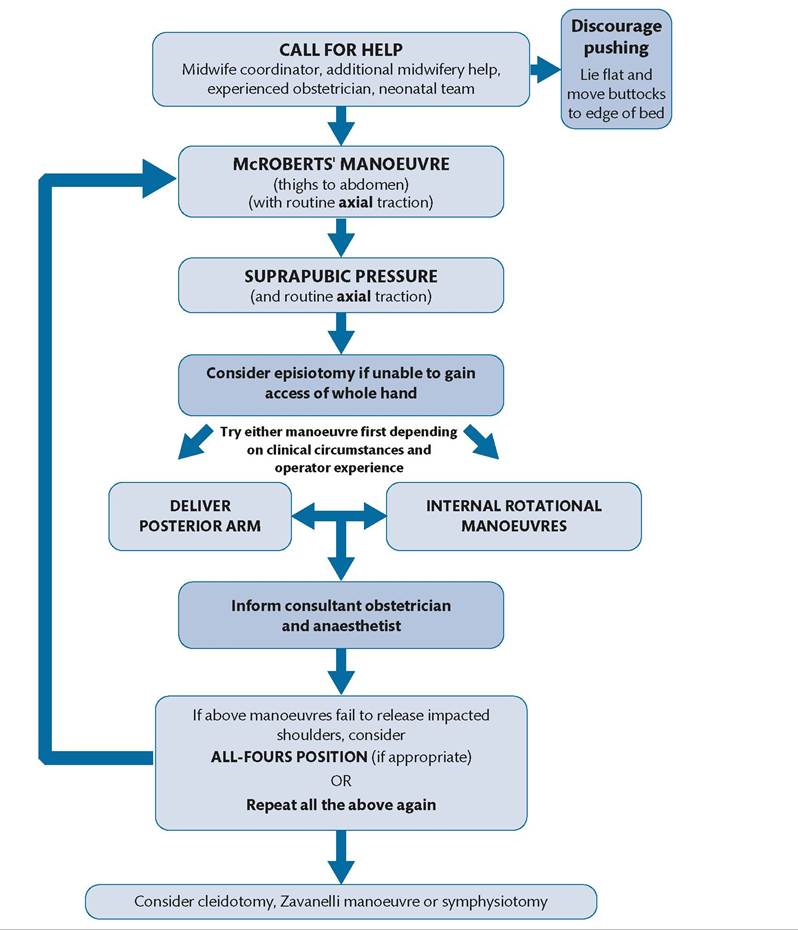
An algorithm for management of shoulder dystocia is displayed in Figure 29.12.
Activate the emergency bell to call for urgent help from the multiprofessional team: senior midwives, experienced obstetricians, and additional maternity staff. Ensure the neonatal team is contacted
Baby to be reviewed by midwife/neonatologist after birth and referred for Consultant Neonatal review if any concerns
DOCUMENT ALL ACTIONS ON PRO FORMA AND COMPLETE CLINICAL INCIDENT REPORTING FORM.
Figure 29.12 Algorithm for management of shoulder dystocia.
Reproduced from Winter C, Crofts J, Laxton C, Barnfield S, Draycott T, (eds.) PROMPT: PRactical Obstetric Multi-Professional Training. Practical locally based training for obstetric emergencies. Course Manual. 2nd edition. Cambridge: Cambridge University Press; 2012.
urgently to support neonatal resuscitation if required, and assess the baby for signs of injury after birth. If shoulder dystocia occurs at home, a paramedic ambulance should be immediately requested.
State the problem clearly: ‘This is a shoulder dystocia’. Take note of the time of birth of the head and, if possible, assign one team member to document timings and actions. Ask the mother to stop pushing, as this will further impact the shoulder against the symphysis pubis and will not resolve the dystocia.
Manoeuvres
Upon diagnosis of shoulder dystocia, the following manoeuvres should be attempted in a stepwise fashion. After each manoeuvre, apply routine axial traction to assess whether the shoulders have released.
If unsuccessful, move on to the next manoeuvre.These manoeuvres must not be attempted ‘prophylactically’ in anticipation of shoulder dystocia, as this will make it difficult to assess if there this was definitely a shoulder dystocia and will impact the management of future births and cause maternal anxiety.
McRoberts' manoeuvre
This simple manoeuvre is an effective intervention, with reported success rates as high as 90% (35). It has a low rate of complication and is one of the least invasive manoeuvres. It should therefore be used first, if possible. McRoberts’ position increases the relative anteroposterior diameter of the pelvis, by straightening the sacrum relative to the lumbar spine and rotating the maternal pelvis towards the woman’s head.
Lay the woman flat and remove any pillows. Bring her to the end of the bed and/or remove the end of the bed to make vaginal access easier. With one assistant on either side, hyperflex the woman’s legs so that her thighs are brought close to her abdomen and her knees are up towards her ears. If the woman is in lithotomy, remove her legs from the supports to achieve McRoberts’ position.
Apply routine axial traction. If the fetal shoulder is not released, move on to the next manoeuvre.
Suprapubic pressure
Suprapubic pressure aims to rotate the anterior fetal shoulder, releasing it from behind the symphysis pubis into the wider oblique diameter of the pelvis.
Identify the location of the fetal back. Ask an assistant to apply pressure just above the symphysis pubis in a downward, lateral direction from the side of the fetal back. If you are unsure of the location of the fetal back, apply suprapubic pressure from the most likely side of the fetal back, and attempt from the other side if this is unsuccessful.
If the fetal shoulder is not released with routine axial traction, stop suprapubic pressure and move on to the next manoeuvre.
Internal manoeuvres
The two internal vaginal manoeuvres are delivery of the posterior arm and internal rotational manoeuvres.
There is no evidence to suggest that one is superior or should be attempted first. Although episiotomy will not relieve the bony obstruction of shoulder dystocia, it can be considered to allow more space to insert the birth attendant’s hand to facilitate these manoeuvres.Both manoeuvres involve gaining access into the vagina. With the woman maintained in McRoberts’ position, the most spacious part of the pelvis is the sacral hollow, posteriorly. There is very little room anteriorly or laterally. The whole hand must be inserted into the vagina, as it is otherwise very difficult to perform the manoeuvres. The technique to insert the hand into the sacral hollow is to scrunch up your hand as if putting on a tight bracelet, as demonstrated in Figure 29.13.
Delivery of the posterior arm
Delivering the posterior arm will reduce the diameter of the fetal shoulders by the width of the arm. The aim is to grasp the fetal wrist and gently withdraw the baby’s hand from the vagina in a straight line. This movement is similar to the action of ‘putting your hand up in class’. Once the posterior arm is delivered, routine axial traction will usually achieve birth of the baby.
Babies often lie with their arms flexed, therefore the fetal wrist may be easily felt when you access the vagina. However, if the posterior arm is lying straight against the body, the fetal wrist may be more difficult to reach. The arm will need to be flexed to bring the wrist closer to you. Follow the posterior shoulder and arm with your hand until you reach the elbow. Place your thumb in the antecubital fossa and apply pressure to the back of the elbow with your fingers. This should flex the posterior arm and allow the wrist to be grasped.
If you cannot reach the wrist, move on to the next manoeuvre. Do not pull on the upper arm as this will not bring the wrist closer and may result in a humeral fracture. If the posterior arm is delivered but the shoulder dystocia has not resolved, support the head and posterior arm and gently rotate the baby through 180 degrees.
This should resolve the shoulder dystocia, as the posterior shoulder will now become the anterior shoulder and should be below the symphysis pubis.Internal rotational manoeuvres
Internal rotational manoeuvres aim to move the fetal shoulders into a wider pelvic diameter. As the fetal shoulders rotate within

Figure 29.13 A demonstration of the technique for inserting the hand into the sacral hollow.
the pelvis, the fetal shoulder descends through the pelvis due to the bony architecture of the pelvis. Internal rotation can be most easily achieved by applying pressure on the anterior (front) or posterior (back) aspect of the posterior shoulder to guide the shoulders into an oblique or transverse diameter. At the same time, an assistant can apply suprapubic pressure to aid rotation of the shoulders. The direction of suprapubic pressure depends upon the direction you are attempting to rotate the shoulders, that is, ensure you are both attempting to guide the shoulders in the same direction. Birth should then be achieved with routine axial traction.
All-fours position
If these manoeuvres do not work, either try all the manoeuvres again or consider the all-fours position, as the change in position may dislodge the anterior shoulder (37). Some midwives may prefer to try the all-fours position prior to internal rotational manoeuvres.
Last-resort options
These include vaginal replacement of the fetal head (Zavanelli manoeuvre) and maternal symphysiotomy. These procedures are rarely required and are associated with serious maternal morbidity (38-41).