Recovery from birth
Vagina, perineum, and pelvic floor
For 2 or 3 days after birth the vagina remains capacious and smooth walled, but after this the characteristic rugae reappear and the vaginal capacity reduces quickly.
During this time there are histological signs of oestrogen withdrawal, with thinning of the squamous lining and absent glycogen storage granules and basal layer activity(1). This state persists for 1 or 2 months, whereupon there are progressive changes in the vaginal skin bringing structure and function closer to the physiological premenopausal state. A complete return to normal epithelial cyclicity and function does not occur until ovulation commences.
Approximately 85% of vaginal births are complicated by perineal trauma, the majority of which will require suturing to repair
(2). In normal circumstances, lacerations, episiotomy, or a combination of the two will heal over 2-3 weeks with healing complete by 4-6 weeks. However, the repair process will be complicated by infection and partial or complete dehiscence in up to 5% of cases. Careful assessment and management of these complications is required since there is a potential for longer-term sequelae such as painful intercourse and incontinence. Complications of perineal injuries have been associated with postnatal depression and longer- term psychological problems. It is important to provide women with information and support regarding perineal care and hygiene, and regular inspection of the region should be undertaken during the early postpartum period.
Vaginal birth may also cause injury to the endopelvic fascia that supports and holds the vagina in position, and there may be injury to the levator plate. Trauma to the levator muscles, such as partial avulsion from the pelvic sidewall, is a recognized cause of pelvic floor dysfunction characterized by prolapse and incontinence (Figure 35.1).
The incidence of such injuries is between 10% and 20% following spontaneous vaginal birth and lift-out ventouse delivery, but may be as high as 30% or more following forceps delivery (3). Although there may be no specific additional treatment when these injuries are present, and indeed they can be difficult to diagnose without recourse to imaging, recognition may help women understand changes in pelvic floor function and allow contact with physiotherapists and others skilled in longer-term maintenance of continence.It has been reported that one or both pudendal nerves are injured during vaginal birth in up to one-third ofwomen (4). Traction injury to the pudendal nerve is associated with incontinence of flatus and sometimes faeces, urinary incontinence and voiding dysfunction, and perineal pain that can lead to sexual difficulties. Fortunately for the majority of women these injuries heal spontaneously although a small proportion of women can have unpleasant symptoms that last for many years.
Caesarean recovery
In many parts of the world, one-quarter or more of births are caesarean and differences in recovery pattern from vaginal birth should be taken into account. Following an uncomplicated caesarean section there is no reason that women should not have a normal oral intake, and early mobilization should be encouraged. Prolonged immobility and dehydration are independent risk factors for thromboembolic complications and should be avoided. Other factors that
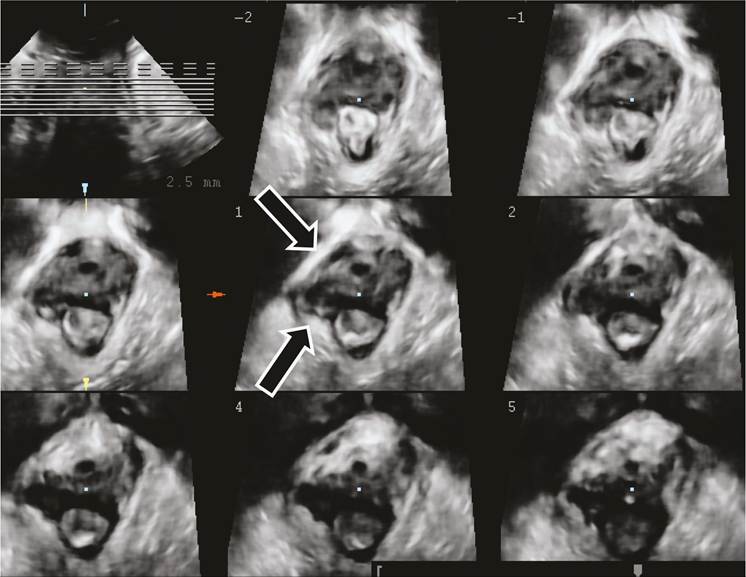
Figure 35.1 Ultrasound image of the pelvic floor in a woman following forceps vaginal delivery, showing avulsion of the levator plate from the right pubic ramus.
Courtesy of Professor HP Deitz.
influence the risk of thrombosis include increasing maternal age, obesity, and inherited thrombophilia: women with these risk factors should be considered for formal anticoagulation in addition to mechanical measures such as compression stockings (5).
Recovery in the first few days after birth tends to be slower than that following an uncomplicated vaginal birth, and this can have adverse effects on a woman's ability to manage and care for the newborn and her older children. The majority of women will develop minor health problems that will require treatment whether delivered by caesarean section or vaginally, but women who have had a caesarean section are less likely to have problems than those with a forceps or ventouse delivery (6).Restrictions on heavy lifting are commonly recommended following caesarean delivery but there is little objective evidence on which to base such advice. It would make sense to reduce activity that might predispose to wound dehiscence or subsequent hernia, but fortunately such complications are rare. An issue of practical concern for many women is driving: advice regarding driving is commonly based on guidelines of insurance companies. When objectively measured, there does not seem to be any difference in women's ability to handle driving irrespective of the mode of birth, and driving seems to be safe from very early in the postnatal period (7). It seems likely that a greater issue is fatigue and its negative effect on driving capacity, with women in the postnatal period subject to sleep deprivation that is likely to have a much greater effect on driving than mode of birth (8).
Uterine involution
When the uterus becomes empty following birth, contraction of the myometrium and continuing uterine tone reduce blood loss. The arterioles and venous channels of the placental bed thread their course through interlacing bundles of uterine muscle, so myometrial contraction acts to compress them. To enhance the mechanical effect of uterine contraction, there are corresponding changes in blood coagulability with a reduction in clotting time and rapid increases in the concentration of clotting factors VIII and V, with a decrease in fibrinogen and a surge in platelet concentration (1).
The uterus reduces in size rapidly, following both vaginal birth (Figure 35.2) and caesarean section (Figure 35.3) reaching prepregnancy dimensions by about 1 month following birth in healthy women. Although it is difficult to obtain tissue for analysis, it seems likely that there is minimal loss of total myometrial cells, but a marked reduction in length and a reduction in the elastin and collagen content of the uterus. The uterine tone is maintained during the early postnatal period although Doppler studies show a steady increase in vascular resistance (1).Large areas of decidua are shed soon after birth, but new endometrium grows from the deeper portions of the endometrial glands that remain in the basal layer, and a relatively complete surface has usually grown within 2 or 3 weeks of delivery (9). The placental site is slower to heal, and the large arcuate arteries that supplied the placenta become hyalinized and endometrial growth encroaches from the peripheral margins of the placental site to cover it. This process
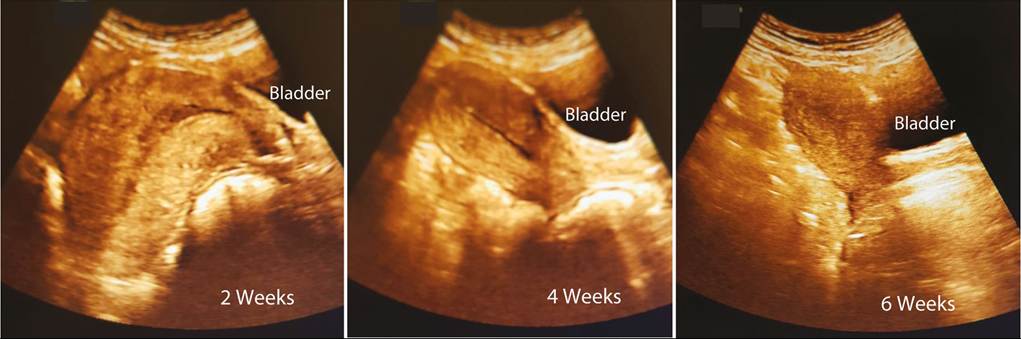
Figure 35.2 Sequential ultrasound images at 2, 4, and 6 weeks postpartum in a primigravid woman, showing involution progressing most rapidly in the first month.
is slow compared to the rest of the uterine surface and can take up to 6 weeks for a full endometrial coverage. The cervix returns to a relatively normal morphology within 2 weeks, although it will have a different shape and characteristics to that of a nulligravid woman.
These physiological changes are characterized by two well-known clinical correlates—Thfterpains' and lochia. So-called afterpains are sensations of uterine contraction similar to, but milder than, uterine contractions. They are typically experienced by multiparous women at the time of breastfeeding, presumably a response to oxytocin release, and may herald transient passage of heavier blood loss or clots. Afterpains typically decrease in intensity and level of pain over the first 2 or 3 postnatal days and are rare thereafter.
‘Lochia' is the vaginal discharge that occurs following birth. It is usually light but frank blood for the first few hours after birth, changing to a brown light fluid discharge until the third postpartum day. This has classically been termed ‘lochia rubra' and contains blood from the placental site, any remaining placental tissue or membranes, some necrotic decidua, and cervical discharge. Beyond the fourth or fifth day the lochia changes to a creamy straw-colour (the ‘lochia serosa') containing serous fluid, leucocytes, and mucus. For another week or two there is a light and clear discharge (the ‘lochia alba') that contains sloughed decidual cells and cervical mucus. At this stage, there is commonly contamination with bacteria which gives the lochia a characteristic smell.Initiation of lactation
The physiological changes necessary for lactation begin in mid pregnancy, and the transition to lactation is completed postnatally. In the prepregnant state the breast has a series of ducts growing inward from the nipple and traversing the fat pad of the breast, ending in terminal duct lobular units. Under the influence of pregnancy- related hormones including prolactin, human placental lactogen, oestrogens, and progesterone, the terminal ductal units grow and expand and from about mid pregnancy some secretory activity begins (10). The initiation of secretory activity in the terminal lobules is termed stage one lactogenesis, but there is a period of quiescence until birth that is likely mediated by the effect of progesterone. With the fall in progesterone after birth, milk secretion begins and continues in response to prolactin. This transition is referred to as stage two lactogenesis, and with the rapid increase in milk production the alveoli express receptors for oxytocin. Triggering of these receptors leads to contraction of the alveolar myocytes, squeezing milk into the ducts of the breast.

Figure 35.3 Sequential ultrasound images at 2, 4, and 6 weeks postpartum in a multiparous woman, showing involution progressing most rapidly in the first month. The area of haematoma and oedema at the site of the uterine incision is arrowed.
More on the topic Recovery from birth:
- CONTENTS
- METABOLIC DISORDERS IN NEWBORN
- TECHNICAL FACTORS OF NEEDLE ELECTROMYOGRAPHY
- Perimortem Cesarean Delivery
- Chapter 21 Gastrointestinal, Renal, and Surgical Complications
- The Red Word ofIvan Kulyk
- Judging and Mediating for the “Long Emergency”
- Reproductive technologies
- ACUTE KIDNEY INJURY
- Chapter 18 Postterm Pregnancy