A standard in vitro fertilization treatment cycle
Patient selection and workup
Perhaps the most important part of an IVF treatment is the work that takes place before the first injection is given. Patients must have a full understanding of what is planned, including the processes involved, their risks and benefits, the likelihood of pregnancy, and the costs involved.
There should be easy access to independent counselling from a trained fertility counsellor and adequate time for reflection and discussion with an accredited clinical specialist before the decision to proceed is taken. The clinician will use markers of ovarian reserve (anti-Mullerian hormone (AMH) and antral follicle count (AFC)) (6, 7) along with patient age and previous history to decide on the dose of follicle-stimulating hormone (FSH) to be used. Various algorithms have been developed to try to optimize FSH dose selection but, to date, they have not gained widespread acceptance.Ovarian stimulation
Two main types of stimulation protocol are widely used in ART clinics. The older Iongprotocol (Figure 52.2) was first developed in the late 1980s and involves pretreatment with a gonadotropin-releasing hormone (GnRH) agonist (e.g. buserelin, nafarelin, or leuprolide) (8) given by injection or nasal spray from the mid-l uteal phase of
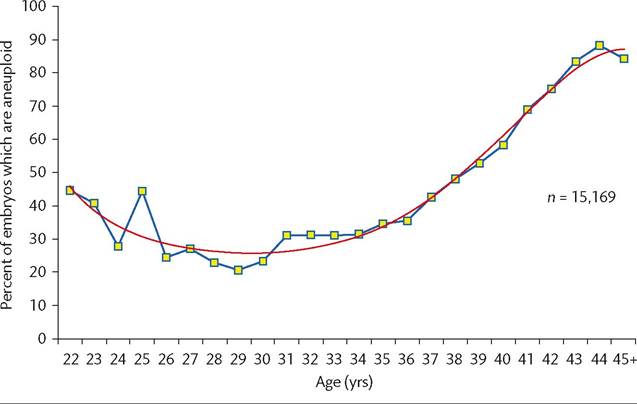
Figure 52.1 Female age and embryonic aneuploidy.
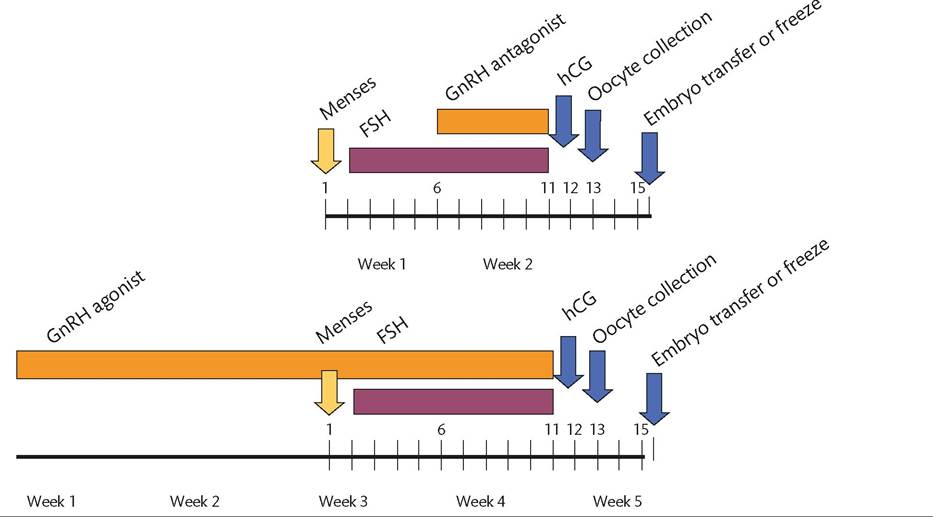
Figure 52.2 Schematic of processes involved in ‘long protocol' GnRH antagonist-controlled and GnRH agonist-controlled ovarian stimulation.
the previous menstrual cycle. Initiation of GnRH agonist treatment at this time induces a short-lived increase (flare) in circulating FSH and LH followed by pituitary downregulation with profound suppression of gonadotropin secretion.
A normal menstrual bleed follows after a few days, at which point a blood sample is taken to check pituitary downregulation and an ultrasound scan is performed to exclude ovarian cysts and check that the endometrium is thin. This is followed by daily injection of exogenous gonadotropin, either a recombinant FSH (Gonal- F, Puregon) or a urinary derived FSH with LH activity (Menopur, Merional). Both types of gonadotropin preparation seem equally effective at stimulating ovarian follicle growth although the manufacturing companies all claim superiority using different methods of assessment and different studies.The purpose of ovarian stimulation is to produce multiple ovarian follicles, allowing collection of multiple oocytes. Different women respond very differently to gonadotropin treatment. Some, mainly older women or those with low AMH and AFC levels, require large doses for adequate stimulation whereas others, younger or with signs of polycystic ovary syndrome, are hypersensitive and at risk of ovarian hyperstimulation syndrome even with modest doses. Hence caution must be exercised when prescribing gonadotropins and the ovarian response must be closely monitored during stimulation. Monitoring is carried out both with transvaginal ultrasound and with measurement of oestradiol in serum. Stimulation should result in growth of a cohort of six to ten large follicles with a concomitant increase in serum oestradiol and endometrial thickness on ultrasound scanning. The average duration of stimulation is between 10 and 12 days although this is also variable.
Once a lead follicle diameter of 18-20 mm is reached, a single injection of human chorionic gonadotropin (hCG) 5000-10,000 IU is given: the ‘hCG trigger’. This induces final oocyte maturation with expulsion of the first polar body. Ovulation will occur 38-42 hours later, so a transvaginal ultrasound-guided oocyte collection is scheduled about 36 hours after hCG, allowing collection of mature oocytes (Q Video 52.1).
hCG has a half-life of several days (9) and, in the presence of an excessive ovarian response to gonadotropin treatment, can initiate a process of ovarian hyperstimulation. This involves capillary endothelial dysfunction, probably mediated by vascular endothelial growth factor (10), leading to leakage of fluids and small molecules out of the vascular compartment, with ascites, pleural and pericardial effusions, and haemoconcentration. Arterial and venous thrombosis can occur and several deaths from severe ovarian hyperstimulation syndrome (OHSS) have been reported. This has led to a reappraisal of the use of the long protocol for stimulation with high-dose FSH and hCG trigger. Introduction of a new class of GnRH antagonists in the late 1990s allowed the long protocol to be replaced with the antagonist protocol. This does not require pretreatment for pituitary downregulation but rather initiates GnRH antagonist treatment on the fifth day of FSH injection (11). Hence, the antagonist protocol is perceived by patients as quicker, with completion of drug treatment within 10-12 days on average. The antagonist protocol is frequently combined with mild stimulation using lower doses of FSH. If there is still excessive follicle growth with high concentrations of oestradiol and risk of OHSS then final oocyte maturation can be induced with a dose of GnRH agonist, an agonist trigger. This releases endogenous LH, mimicking the natural LH surge (12). This approach cannot be used in the long protocol as the pituitary is desensitized to GnRH so no LH would be released. Agonist trigger has almost completely removed risk of OHSS, leading to the concept of the ‘OHSS-free clinic’ (13), placing safety as of equal importance to efficacy in IVF practice.
Oocyte and sperm collection
Transvaginal ultrasound-guided oocyte collection can usually be carried out with light sedation rather than general anaesthesia, and involves passage of a needle through the lateral vaginal fornix and into the nearest follicle under ultrasound guidance (Q Video 52.1).
Although not entirely free of a risk of infection, bleeding, or perforation of an abdominal structure, the procedure is low risk and usually takes 15-20 minutes to perform. The procedure can be made more complicated if there is significant endometriosis or pelvic adhesions or if the ovarian response is low.IVF requires both oocytes and sperm. Collection of sperm is usually by masturbation, with subsequent resuspension of the semen sample in culture medium and separation of sperm by centrifugation. Cases in which ejaculation of sperm cannot be achieved, for example, after vasectomy or in the presence of blockage or absence of the vas deferens, can be managed by testicular sperm extraction or percutaneous epididymal sperm aspiration, or occasionally by open surgery. Sperm are either incubated with the oocyte in a drop of culture medium, for IVF, or a single sperm is microinjected into the oocyte by ICSI if sperm number or motility is poor. Some studies have associated pregnancies conceived after ICSI, but not IVF, with increased risks of abnormality in the offspring and the excessive use of ICSI, particularly for non- male factor infertility, is discouraged (14).
Embryo growth and development
Traditionally, the early division of the embryo has been monitored by removal of the dish containing the embryos from the incubator once per day with analysis of embryo morphology by light microscopy. This disturbs the equilibrium of the embryo, with cooling and loss of oxygenation and buffering. The recent introduction of video time-lapse embryo assessment allows real-time monitoring of embryo growth using a video clip derived from still photographs taken every few minutes by a camera within the incubator (15) (Q Video 52.2). This gives a more detailed picture of the development of the embryo, which can be assessed in comparison with optimal developmental stages as a measure of the quality of the embryo. Such an assessment should provide a more rational basis for selection of the best embryo to transfer, although randomized trials demonstrating improvement in live birth rate are still awaited.
In the early days of IVF, the laboratory environment was severely suboptimal for embryo growth and embryos were transferred to the uterine cavity after 2 days, just sufficient time to confirm viability. Early embryo transfer does not allow any assessment of quality, leading to low pregnancy rates per cycle. More recent improvements in culture media and incubators have allowed high rates of embryo development to blastocyst stage, involving 5 days of culture in vitro (Figure 52.3). Prolonged culture permits a detailed comparison of embryos within one cohort, with selection of the best quality for transfer and for cryopreservation. This policy has dramatically improved success rates and has allowed clinics to reduce the number of embryos transferred per attempt, such that most women under 40 will have a single embryo transfer (SET) in many of the most advanced centres (16). Avoidance of multiple pregnancy, with a fivefold reduction in risk of premature birth and handicap, has become one of the most important targets for ART in the twenty-first century. While multiple pregnancy rates of less than 5% per cycle are reported from Scandinavia and Australia, rates in excess of 10%
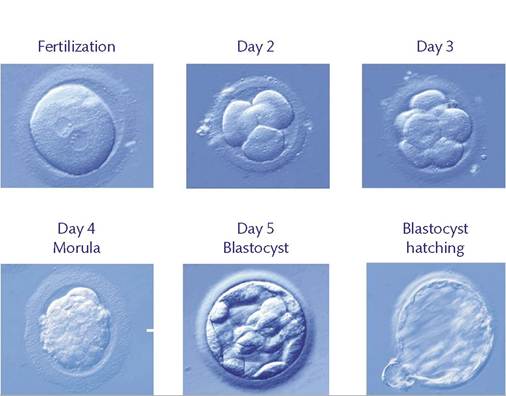
Figure 52.3 Human embryo development from fertilization to blastocyst.
are still seen in the United Kingdom and 30% in the United States. Premature birth imposes significant burden on parents and financial cost to society, and rates can only be reduced by increasing utilization of SET (18). Recent improvements in pregnancy rates after transfer of a single frozen-thawed embryo (19) have given further encouragement to patients to accept a fresh SET, since the cumulative chances of pregnancy with fresh plus frozen embryo transfer are equivalent or better than those seen with fresh transfer of two embryos.
Embryo transfer
A standard embryo transfer involves visualization of the ectocervix using a vaginal speculum followed by insertion of a fine plastic cannula through the cervix to the uterocervical junction.
The embryo selected for transfer is then drawn into a narrower flexible transfer catheter. This runs along the outer cannula to pass into the endometrial cavity, at which point the embryo is expelled in a drop of culture medium. The procedure takes a few minutes and is frequently carried out using transabdominal ultrasound to ensure correct catheter placement and to visualize expulsion of the drop of medium containing the embryo (Q Video 52.3). Problems can occur when there is cervical stenosis, for example, after previous surgery, and a precycle hysteroscopy and cervical dilation may need to be considered for the next cycle after a difficult transfer.Transfer of frozen embryos can be performed using a natural or medicated transfer cycle. Most clinics will use the woman's natural cycle if she is regularly ovulating and has good endometrial development on ultrasound scanning. The patient will have monitoring with blood or urine testing for the LH surge and postsurge rise in progesterone, demonstrating that natural ovulation has occurred. Ultrasound is used to confirm development of the corpus luteum and that endometrial thickness is adequate (>6 mm). The day for embryo transfer is then calculated depending on whether the embryo was frozen on day 2, 3, or 5. Transfer technique is as for fresh transfer, but luteal support is not necessary. Women who are anovular or who have poor endometrial development can either use ovulation induction with clomiphene citrate or FSH injection to induce natural ovulation with endometrial development, or can use an artificial cycle with treatment first with oestradiol valerate or oestrogen patch, followed by progestogens.
Luteal phase
Luteal phase support, in the form of either hCG injections or pro- gestogens, is widely used in both long and antagonist protocols. The natural development of the corpus luteum does not occur efficiently after ovarian stimulation and implantation rates after embryo transfer are low if some type of support is not used. Pregnancy rates appear similar whether hCG or progestogens are employed, but hCG injection can worsen symptoms of OHSS so has largely been superseded in modern practice (19). Progestogens are given as a vaginal pessary (Uterogestan), gel (Crinone), or tablet (Endometrin), or by deep intramuscular injection. While many clinics discontinue luteal progestogen when the pregnancy test is positive, others will continue with this support for many weeks. The impact on the likelihood of viable pregnancy of this latter approach is questionable.
Pregnancy testing is by measurement of hCG in serum 10- 14 days after embryo transfer. A negative test is followed by cessation of luteal support and by menstruation. It is usual to wait for one further menstrual cycle before beginning stimulation again although some women prefer to carry straight on to another cycle if there has not been ovarian hyperstimulation. A positive test is usually repeated a few days later to monitor the rise in hCG and progesterone, followed by an early pregnancy transvaginal scan at 2-3 weeks after the positive pregnancy test. This first ultrasound scan should demonstrate fetal viability with the presence of a heartbeat, and confirm that the pregnancy is intrauterine (not ectopic) and singleton. Suspicion of miscarriage should trigger further assessment by ultrasonography a few days later rather than early intervention which may inadvertently terminate an early healthy gestation.
Potential IVF patients want to know their chance of having a healthy child from their cycle of treatment. Hence, the best measure of ‘success’ from a patient perspective is the live birth rate per cycle started. This is defined as the start of FSH injection and takes into account all of the things that can go wrong in an IVF cycle, including failure of the ovaries to respond to stimulation, or overstimulation leading to cycle cancellation, failure of fertilization, failure of implantation, miscarriage, or ectopic pregnancy. This statistic has been championed by the United Kingdom Human Fertilisation and Embryology Authority (http://www.hfea.gov.uk) and forms the basis of their comparative statistics. However, even this can be challenged. As mentioned previously, best practice in IVF may now be use of an antagonist protocol with agonist trigger and freezing of all embryos in order to minimize risk of OHSS. If this approach is followed then the live birth rate per cycle started must include births following transfer of both fresh and frozen embryos derived from the initial stimulation. This ‘cumulative conception rate’ becomes the most relevant global static but will only be known many months after the start of stimulation, given the delays inherent in utilization of frozen embryos (20). Hence live birth rate per fresh transfer is more often quoted.
Clinics must audit their practice and a number of other markers of success are relevant in this context. The implantation rate—rate of positive pregnancy test per embryo transferred—is the best marker of quality of the embryology laboratory, and clinical pregnancy rate—defined as the rate of observed fetal heart activity on early scan per embryo transferred—is also relevant. However, these measures do not take into account any problems with under- or over-response to stimulation and any statistic quoted with ‘per embryo transfer’ as the denominator should be viewed with suspicion when clinic success rates are quoted.