Vulva
Malignant tumours and premalignant conditions
Squamous cell carcinoma
Carcinoma of the vulva accounts for 3% of all female genital cancers and occurs mainly in women aged over 60 years.
Squamous cell carcinoma is the most common type (86%). These tumours are divided into two groups: keratinizing squamous cell carcinomas unrelated to human papillomavirus (HPV) (>70% of cases), and warty and basaloid carcinomas, which are strongly associated with high-risk HPV (<25% of cases), mainly HPV16 (1, 2).Aetiological factors and precursor lesions
Keratinizing squamous carcinomas frequently develop in older women (mean age 76 years), sometimes in the context of longstanding lichen sclerosus. The precursor lesion is referred to as differentiated vulval intraepithelial neoplasia dVIN or VIN simplex (Figure 70.1a), which carries a high risk of cancer development. In contrast, the less common HPV-associated warty and basaloid carcinomas develop from a precursor lesion called squamous intraepithelial lesion (SIL) VIN comprising a spectrum of alterations ranging from low-grade SIL VIN (VIN1) to high-grade SIL VIN (VIN 2-3) (Figure 70.1b). Recent proposals from both the International Society for the Study of Vulvovaginal Disease (ISVVD) and the College of American Pathologists (CAP)ZAmerican Society for Colposcopy and Cervical Pathology (ASCCP) have recommended replacement of the older three-tiered system (VIN 1-3) used to describe these lesions with a two-tiered system. HPV-associated SIL VIN lesions have a low risk of progression to invasive carcinomas (approximately 6%), except in older or immunosuppressed women (1, 2).
Pathology
SIL VIN may be single or multiple, and macular, papular, or plaque-like. Histological grades are labelled low-grade SIL VIN I, corresponding to mild dysplasia, and high-grade SIL (VIN 2-3) corresponding to, moderate, and severe dysplasia, respectively.
However, high-grade SIL (VIN 3)—which includes squamous cell carcinoma in situ (CIS)—is by far the most common.Keratinizing squamous cell carcinomas usually follow differentiated VIN (VIN simplex). Most tumours are exophytic but some may be ulcerative. Microscopically, the tumour is composed of invasive nests of malignant squamous epithelium with central keratin pearls (Figure 70.2). The tumours grow slowly, extending to contiguous skin, vagina, and rectum. They metastasize initially to superficial inguinal lymph nodes, and then to deep inguinal, femoral, and pelvic lymph nodes (1, 2).
Clinical features
Prognosis correlates with stage of disease and lymph node status. The number of inguinal lymph nodes with metastases is the most important single factor. The International Federation of Gynecology and Obstetrics (FIGO) staging of vulval cancer defines tumors of any size limited to the vulva as Stage I carcinomas; tumors extending to adjacent perineal structures (lower one-third of the urethra, lower one-third of the vagina, or anus) as Stage II; tumors with positive inguinofemoral lymph nodes as Stage III; and tumors invading the upper two-thirds of the urethra, upper two-thirds of the vagina, distal structures, or distant metastasis as Stage IV. Tumor grade and number, size, and location of lymph node metastases determine survival. Well-differentiated tumors have a better mean survival, approaching 90% if nodes are negative. Two-thirds of women with inguinal node metastases survive 5 years, but only one-fourth of those with pelvic node metastases live that long (1).
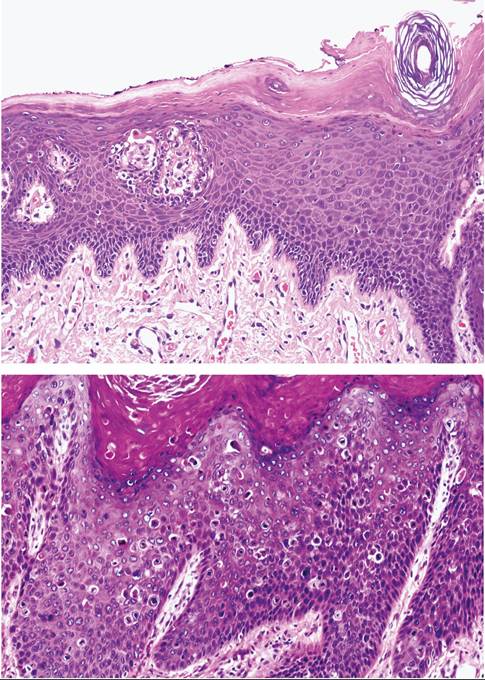
Figure 70.1 Vulval intraepithelial neoplasia (VIN). (a) Well-differentiated (simplex) type. The atypia is accentuated in the basal and parabasal layers. There is striking epithelial maturation in the superficial layers. (b) HPV- related undifferentiated (classic) VIN. Beneath a hyperkeratotic surface the epithelial cells are atypical.
There are numerous mitoses.Verrucous carcinoma
Vulval verrucous carcinoma is a distinct variety of squamous cell carcinoma that manifests as a large fungating mass resembling a giant condyloma acuminatum. HPV, usually type 6 or 11, is commonly identified. The tumour invades with broad tongues. Verrucous
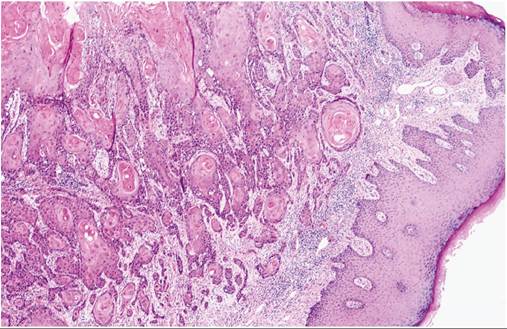
Figure 70.2 Keratinizing squamous cell carcinoma of the vulva. Nests of neoplastic squamous cells, some with keratin pearls, are evident.
carcinomas rarely metastasize. Wide local surgical excision is the treatment of choice.
Basal cell carcinoma
Basal cell carcinomas of the vulva are identical to their counterparts in the skin. They are not associated with HPV, rarely metastasize, and are usually cured by surgical excision.
Malignant melanoma
Although uncommon, malignant melanoma is the second most frequent cancer of the vulva (5%). It occurs in the sixth and seventh decades but occasionally is found in younger women. It is highly aggressive, and the prognosis is poor.
Extramammary Paget's disease
The disorder usually occurs on the labia majora in older women. The lesion is large, red, moist, and sharply demarcated. The origin of the diagnostic cells (Paget cells) is controversial: they may arise in the epidermis or epidermally derived adnexal structures.
Intraepidermal Paget’s disease may have been present for many years and is often far more extensive throughout the epidermis than preoperative biopsies indicate. Unlike Paget’s disease of the breast, which is almost always associated with underlying duct carcinoma, extramammary Paget’s disease is only rarely associated with carcinoma of the skin adnexa. Metastases rarely occur, so treatment requires only wide local excision or simple vulvectomy (1, 2).