ANTI-BACTERIAL THERAPY
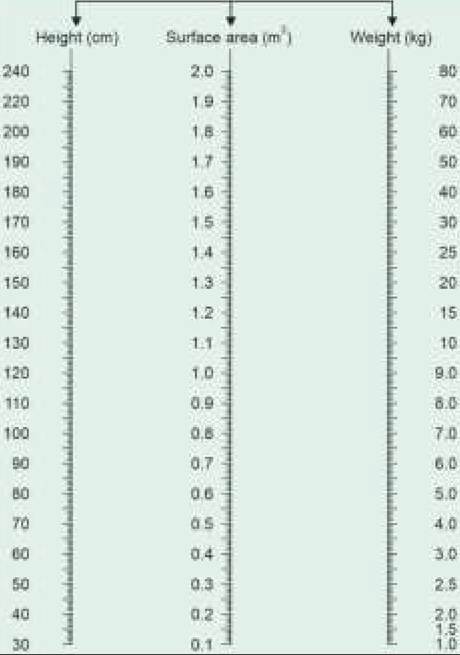
Choice of the antibiotics in bacterial infections depends on causative organism, site and severity of infection, in vitro sensitivity results and patient's characteristics, e.g. age, hepatorenal status, etc.
#946;-lactam antibiotics are those antibiotics which exert antibacterial activity via a #946;-lactam ring in their structure, e.g. penicillins, cephalosporin, monobactum and carbapenems. These antibiotics are rapidly inactivated by #946;-lactamase enzymes, e.g. Penicillinase, cephalosporinase, etc. produced by some pathogens.
Majority of gram-negative bacteria, staphylococci, anaerobes and even mycobacteria produce these enzymes. Consequently, #946;-lactam antibiotics are ineffective against these pathogens, unless combined with a #946;-lactamase inhibitor, e.g. clavulinic acid, sulbactum or Tazobactum. Streptococci, pneumococci and most enterococci do not produce #946;-lactamase enzymes.
Penicillin group of antibiotics contain a common nucleus (6-aminopenicillanic acid) and include Natural penicillins as well as Semi-synthetic penicillins. Benzyl penicillin was the earliest discovered antibiotic extracted from a natural fungal source by Sir Alexander Fleming in 1924.
Mechanism of Action (MoA): All Penicillins are bactericidal, inhibiting cell wall synthesis or activating the enzymes that destroy bacterial cell walls. All of them are #946;-lactam antibiotics (penicillinase-sensitive), except methicillin and its derivatives, e.g. cloxacillin and ticarcillin.
Antimicrobial spectrum:
• Natural penicillin and its repository preparations have narrow spectrum of activity against gram-positive cocci and bacilli,gram-negative cocci, anerobes and spirochetes. These drugs are ineffective against gram negative bacilli and penicillinase-producing pathogens.
• Broad-spectrum penicillins also cover gram-negative bacilli but not the penicillinase-producing organisms, unless combined with a #946;-lactamase inhibitor.
Ampicillin is the drug of choice for Listeriosis.• Penicillinase-resistant penicillins, e.g. cloxacillin are mainly used against coagulase-positive staphylococci. However, these agents are ineffective against Coagulase-negative staphylococci (CONS) and enterococci.
• Extended-spectrum penicillins are highly effective against pseudomonas and anerobic infections but less effective against gram-positive infections, specially staphylococci.
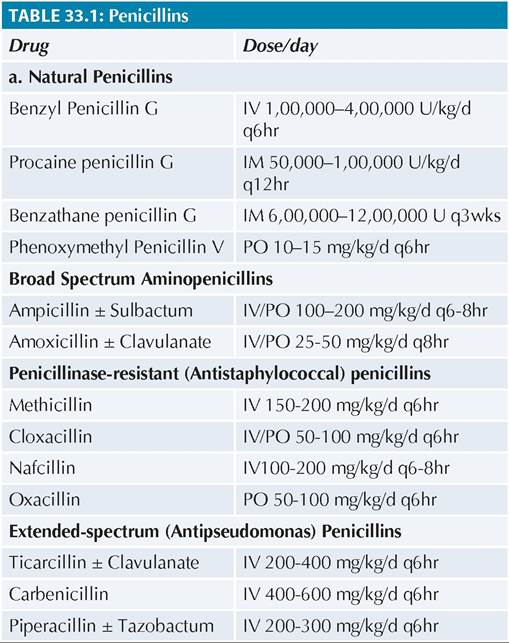
Doses: See Table 33.1.
Adverse-effects (AE): Anaphylaxis is the most serious adverse event of parenteral natural penicillins (~ 1%) and an intradermal sensitivity test is advised before these injections.
Minor hypersensitivity reactions, e.g. urticaria or rash, are common with other penicillins as well but anaphylaxis is rare and sensitivity test is not indicated. However, these drugs should be avoided in cases with history of penicillin allergy. A generalized maculopapular rash is common with ampicillin, specially when used in cases of Infectious mononucleosis or other viral infections.
Drug-induced diarrhea due to altered colonic flora is common, specially with ampicillin, which may
Note: All IV drugs may also be given IM.
be minimized by simultaneous probiotic therapy. Pseudomembranous colitis is a rare complication of ampicillin therapy.
Cephalosporins include antibiotics with a common nucleus (7-Aminocephalosporanic acid). Although penicillinase-resistant, these antibiotics are inactivated by other #946;-lactamase enzymes, e.g. cephalosporinase.
MOA: All cephalosporins are bactericidal, inhibiting cell wall synthesis.
Antimicrobial spectrum:
• First-generation cephalosporins have a microbial spectrum similar to penicillins, while second-generation cephalosporins have greater activity against gramnegative bacilli. Both first and second generation cephalosporins (except cefuroxime) do not cross bloodbrain barrier and hence, ineffective in CNS infections.
• Third-generation cephalosporins have broader spectrum, but with limited activity against staphylococci. These agents cross blood-brain barrier and commonly used for CNS infections.
Fourth-generation cephalosporins have enhanced activity against pseudomonas and staphylococci but do not cover anerobes.
Fifth-generation cephalosporins are broad-spectrum, but predominantly used for methicillin-resistant Staph.
aureus (MRSA) in cases with renal dysfunction, when vancomycin/Teicoplanin cannot be used.
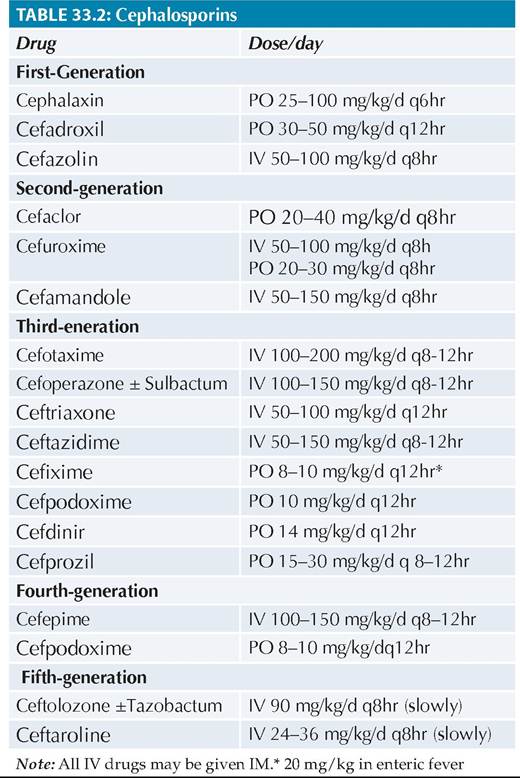
Doses: See Table 33.2.
AE: About 10% of penicillin-allergic patients show crosssensitivity to cephalosporins, which should be avoided in these cases.
Other important adverse effects include—(a) diarrhea, (b) drug fever and (c) nephrotoxicity with some parenteral cephalosporins. These agents should be used with caution in cases with renal damage or coaminoglycoside therapy.
Glycopeptide antibiotics (Vancomycin and Teicoplanin) are commonly used anti-staphylooccccal agents, specially in cases allergic to penicillins/cephalosporins. Teicoplanin is longer-acting and less nephrotoxic than vancomycin.
MoA: These antibiotics are bactericidal by inhibiting cell wall synthesis like penicillins/ cephalosporins, but do not contain #946;-lactam ring.
Spectrum: Apart from excellent activity against staphylococcal infections including MRSA, these antibiotics
also covers gram-positive cocci and bacteria, gramnegative cocci and gram-positive anerobes. Gramnegative bacilli and anerobes are usually resistant to them. These antibiotics are also preferred for:
(a) CSF shunt infections (due to Staph. epidermidis),
(b) pseudomembranous colitis (due to C. difficile), and
(c) infections in neutropenic hosts
Doses:
• Vancomycin IV 40-60 mg/kg/d q6-8 hr
• Teicoplanin IV 10 mg/kg/dose 12-hrly ? 3 doses, followed by 6-10 mg/kg/d q24hr
AE: Nephrotoxicity, Red-man syndrome (Generalized flushing and erythema), Hypersensitivity reactions, Thrombophlebitis.
Aminoglycosides are natural (Gentamicin) or semisynthetic (amikacin) drugs, which are not absorbed orally and hence, given parenterally. Some aminoglycosides, e.g. Neomycin, are used only topically or given orally for bowel sterilization.
MoA: Aminoglycosides are bactericidal, which inhibit or alter bacterial protein synthesis. Natural resistance to these antibiotics is common due to mutations in the organisms.
Spectrum: Aminoglycosides are highly effective against gram-negative bacilli and mycobacteria, but with poor coverage against other aerobes/anerobes. Hence, these agents are often used in combination with penicillins or cephalosporins. Some aminoglycosides are also effective against penicillinase-producing staphylococci.
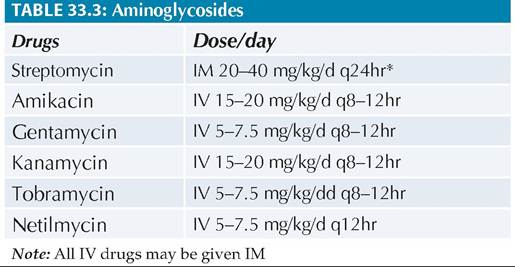
Doses: See Table 33.3. However, these aminoglycoside doses needs modification according to serum creatinine levels in cases with renal damage.
AE: Vestibule-cochlear damage and Nephrotoxicity are most serious adverse events with aminoglycoside therapy. Vestibular toxicity (vertigo) is predominant with streptomycin, while other aminoglycosides predominantly cause cochlear damage on prolonged use (deafness).
Other important adverse events include rashes, drug fever (5%) and rarely, skeletal muscle weakness.

*PO#8725;IV 20 mg/kg/d q12-24hr in enteric fever
**Also used for MAC prophylaxis (PO 15-20 mg/kg/week).
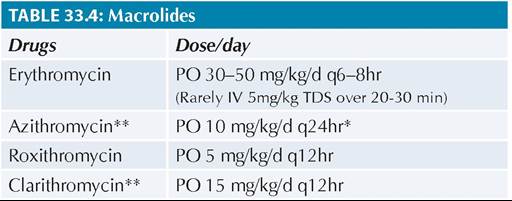
Macrolides antibiotics are almost always used orally and include short-acting Erythromycin or longer-acting Roxythromycin or Azithromycin, etc.
MoA: All Macrolides are bacteriostatic, which act by inhibiting protein synthesis.
Spectrum: These agents are specially active against gram-positive cocci, mycoplasma, chlamydial and treponemal infections. Generally used as oral alternatives to penicillins. Azithromycin is also effective against some gram-negative organisms, including enteric fever.
Spiramycin is a weak macrolide, used mainly for toxoplasmosis. Clarithromycin is also used for prophylaxis against Mycobacterium avium complex (MAC) in immunocompromized children.Doses: See Table 33.4
AE: Gastrointestinal upset, e.g. gastritis/vomiting, and Hepatotoxicity (intrahepatic cholestasis) are predominant adverse events of macrolides,These agents slow-down aminophylline metabolism and should be used with caution in cases on amiophylline.
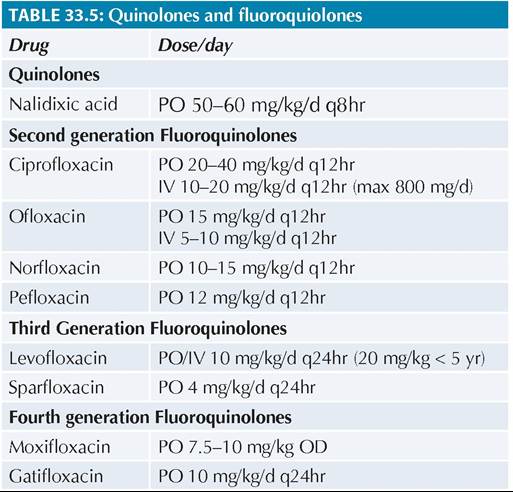
Quinolones and fluoroquinolones include four different generations of antibiotics, of which only first two are generally used in children, specially for enteric fever, urinary tract infections, bacterial diarrhea. Newer generation Levofloxacin and Moxifloxacin are cornersone of treatment for MDR-TB, though resistance to them is also emerging.
MoA: Quinolones are bactericidal, preventing nucleic acid synthesis by inhibiting some enzymes required for maintenance of microbial DNA structure.
Spectrum: These agents are broad-spectrum, effective against both gram-negative and gram-positive pathogens, including those resistant to penicillins, cephalosporins and aminoglycosides. Quinolones are also effective against mycobacteria but with poor activity against anerobes and MRSA infections.
Doses: See Table 33.5.
AE: GITupset, Arthropathy. Potential risk of damage to growing articular cartilage is the major concern for wider use of quinolones, which should be avoided in younger children except as second-line drugs.
Tetracyclines are used sparingly in children due to potential risk of drug deposition in teeth and bones, leading to dental staining, enamel hypoplasia and stunting.
MoA: Tetracyclines are bactericidal drug, inhibiting bacterial protein synthesis.
Spectrum: Although broad-spectrum, tetracyclines are used for limited indications in children, e.g. cholera, plague, Leptospirosis and Rickettsial fevers (drug of choice). Tigecycline is a newer tetracycline, also effective against MRSA and resistant nosocomial infections with E.coli and Klebsiella.
MoA: Carbapenem are potent bactericidal agents, inhibiting cell wall synthesis
33.2
More on the topic ANTI-BACTERIAL THERAPY:
- The Use of Anti-Mycobacterial Therapy for Treatment of Crohn’s Disease
- Carbapenems
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Microbiology of Otitis Media
- Clinical Treatment Trial for Pruritus
- Skin, Soft-Tissue, and Bone Infections Purulent Skin and Soft-Tissue Infections (Furuncles, Carbuncles, Abscesses)
- Anti-Semitic Tracts
- INFECTIVE ENDOCARDITIS
- Appendix Ear Product Formulary