BRONCHIECTASIS
Bronchiectasis is a chronic suppurative lung disease, characterized by ‘-permanent dilatation of the subsegmental airways, due to inflammatory destruction of bronchial/ peribronchial tissue and accumulation of infected material in dependent bronchi'.
Etiopathogenesis: Persistent infection and/or bronchial obstruction are two important events in bronchiectasis. Whole pathology may be initiated by:
• Primary infective lesions, leading to bronchiolar destruction and secondary dilatation in:
± Airway infections, e.g. bronchitis, cystic fibrosis.
± Parenchymal infections, e.g. pneumonia, pertussis, measles.
± Recurrent aspirations and infections, e.g. in GERD, cleft palate, etc.
± Immunodeficiency states
• Primary obstructive lesions with bronchial dilatation, distal collapse and secondary infection in:
± Intrabronchial foreign body, mucus plug, etc.
± Extrabronchial lymph nodes, tumors, etc.
± Functional obstruction, e.g. bronchomalacia, etc.
• Congenital bronchiectasis is seen in:
± Kartagener syndrome, (bronchiectasis, sinusitis and situs inversus).
± Cystic diseases of the lung.
Tuberculosis and foreign body aspiration are two leading causes of bronchiectasis in Indian children, while cystic fibrosis dominates in developed countries.
Pathologically: Bronchiectasis is characterized by- (a) loss of normal ciliated epithelium in bronchi with peribronchial inflammation, (b) thickening and cystic dilatation of bronchi that may be cylindrical, fusiform or secular, and (c) obstructive endarteritis and multiple abscesses.
Right lower-lobe bronchiectasis is common following foreign body aspiration, while tuberculosis usually involves right middle lobe due to bronchial compression by hilar lymph nodes.
Clinical presentation is usually insidious with waxing and waning course. Preceding history of pneumonia, foreign body aspiration or asthma is common.
Important clinical features include:• Persistent wet cough with copious mucopurulent sputum, more prominent in morning due to change of posture causing movement of the mucus and mucosal irritation. Intermittent blood-streaked sputum or frank hemoptysis is not uncommon.
• Failure to thrive and clubbing.
• Respiratory finding, often limited to coarse crepitations or signs of atelectasis.
Diagnosis should be suspected in any case with chronic lung disease and clubbing, confirmed by:
• X-ray chest, showing characteristic honeycomb appearance with/without collapse and multiple small abscesses (Fig. 16.12).
• High-resolution CT scan, which is the gold standard for diagnosis as well as to assess the status of other lung, before surgery. Findings may vary according to pathological type, e.g. tram-lines or signet-ring appearance in cylindrical disease, beaded bronchi in varicose disease and cystic strings and clusters in saccular disease.
• Sputum examination, which is usually seropurulent and separates in 3 layers after few hours-a thin serous layer on top, a fibrinous layer in middle and a cellular layer at the bottom of sample (three-layer test). Direct gram/
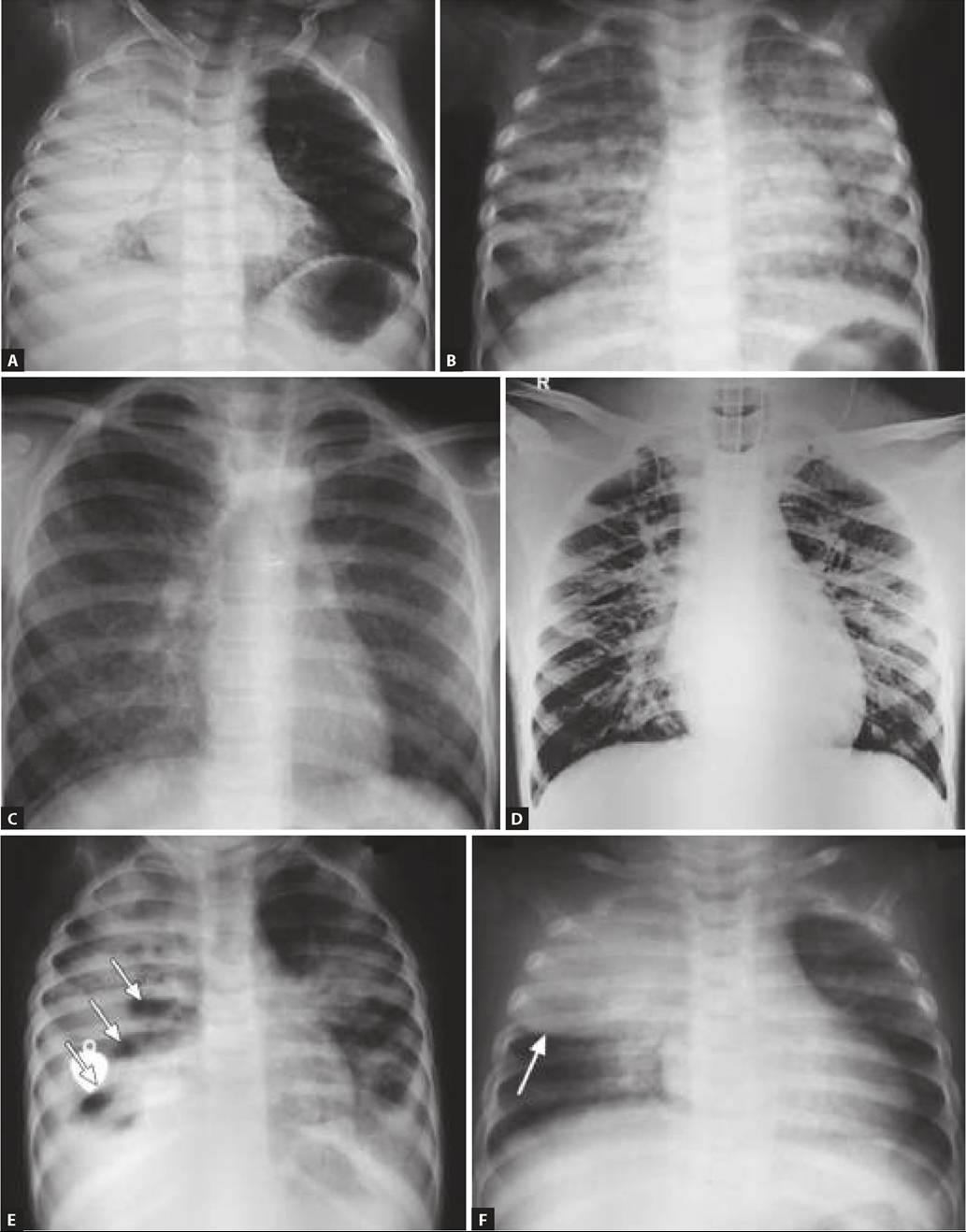
Fig. 16.12: Bronchiectasis (right lower zone): Honey-comb appearance on X-ray chest and HRCT (Inset).
AFB staining and culture of sputum, gastric lavage or brochoalveolar lavage is necessary to establish infective etiology.
• Bronchoscopy is indicated in selected cases to: (i) visualize and remove any obstructive cause, e.g. foreign body, (ii) collect bronchoalveolar aspirate for microbiology, and (iii) bronchial washing or toilet.
• Other relevant etiological investigations, e.g. tuberculin test, sweat chloride test, etc.
Management of bronchiectasis includes:
• Effective clearance of mucus by regular postural drainage, chest physiotherapy and bronchoscopy, if necessary. Airway hydration with inhaled hypertonic saline may improves quality of life in older children.
• Elimination of infective foci by systemic antibiotics, e.g. Coamoxclav during acute exacerbations for 2-3 weeks. Antibiotics should not be used indiscriminately and for prolonged duration, to avoid development of resistant infections. However, long-term prophylaxis with oral (macrolide) or nebulized antibiotics, (e.g. tobramycin, colistin, aztreonam) may be beneficial in selected cases.
• Surgical resection of affected segment is indicated in persistent localized bronchiectasis, while even lung transplant must be considered in severe bilateral disease.
• Immunization for common respiratory infections, e.g. influenza, pneumococci, etc. is recommended in all cases.
16.10.2
More on the topic BRONCHIECTASIS:
- Etiopathogenesis
- DIPHTHERIA
- Interstitial Lung Disease
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Immunodeficiency