Frequently Cited Deficiencies Regarding Specialty Teams
Deficiencies are areas that do not meet compliance with the accreditation standards. In reviewing many specialty teams over the past 20 years, the following list of standards represent the most frequently cited contingencies found among neonatal and pediatric teams.
Accreditation Standard 01.09.01 Physical well-being is promoted through: 3. Protective clothing and dress code pertinent to:
b. Safe operations, which may include the following, unless specified as “required” below:
• Boots or sturdy footwear for on-scene operations (required)
• Wearing reflective material or striping on uniforms for night operations
• High visibility reflective vests or appropriate Department of Transportation (DOT) approved clothing must be worn by flight and ground crews according to the ANSI-SEA 107 standard or equivalent national standard (required)
• Flame-retardant clothing
• Appropriate outerwear pertinent to survival in the environment (required)
• Flight helmets—required for all crews including specialty teams (RW) In addition to wearing helmets, specialty teams frequently do not follow
the dress code of the regularly scheduled team. Wearing scrubs and unsuitable footwear is not appropriate in the event of an unexpected landing or survivable crash in rough terrain and weather.
Accreditation Standard 04.03.05 Securing equipment and supplies—All aircraft equipment (including specialized equipment) and supplies must be secured according to national aviation regulations. (Use of bungee cords is not considered appropriate when securing equipment and supplies). Ambulance equipment must be secured by an appropriate clamp, strap, or other mechanism to the vehicle or stretcher/incubator to prevent movement during a crash or abrupt stop.
All equipment and supplies must be secured. Often, teams have a tendency to store a supply bag under a stretcher without securing it with an appropriate tie-down and even more frequently, medical teams forget that unsecured equipment or supplies in an ambulance can be just as lethal as in an aircraft.
Accreditation Standard 04.03.08 Use of occupant restraint devices:
1. Air medical personnel must be in seat belts (and shoulder harnesses if installed) that are properly worn and secured for all takeoffs and landings according to national aviation regulations. A policy defines when seat belts/shoulder harnesses can be unfastened. (RW/FW)
2. Ambulance personnel must be seat belted when the ambulance is in motion unless emergent patient condition precludes it. (G)
a. Front-seat occupants must always be belted.
b. Overhead grab rails must be present in the patient care area.
c. It is strongly encouraged to have forward and aft facing individual seats. Side-facing bench seats are not recommended. If the ambulance has side-facing bench seats, seat belt mountings must be situated at the pelvic level to restrain personnel/passengers. Shoulder harnesses should not be used on side-facing bench seats.4
Most personnel remember or are reminded by the pilot to fasten restraints in a helicopter or airplane, but many in the back of the ambulance forget to wear seatbelts or choose not to wear them because of the interior design (unable to perform patient care if restrained).
Accreditation Standard 04.02.01 Education Specific to the In-Flight and Ground Transport Environment
1. Completion of all the following educational components should be documented for each of the flight medical personnel. These components should be included in initial education as well as reviewed on an annual basis with all regularly scheduled, part-time, or temporarily scheduled medical personnel and specialty care providers as appropriate for the mission statement and scope of care of the medical service.
a. Medical patient transport considerations (assessment/treatment/ preparation handling/equipment)
b. Day- and night-flying protocols
c. Emergency medical services (EMS) communications (radios) and familiarization with EMS system
d. Extrication devices and rescue operations (ranging from familiarity to explicit training depending on the service's mission statement) (RW)
e.
General aircraft safety. (It is strongly recommended to have the aircraft physically present when providing this training.) This training addresses: (RW/FW)• Aircraft evacuation procedures (exits and emergency release mechanisms) to include emergency shutdown of engines, radios, fuel switches, electrical and oxygen
• Aviation terminology and communication procedures to include knowledge of emergency communications knowledge of emergency communications frequency
• In-flight and ground fire suppression procedures (use of fire extinguishers)
• In-flight emergency and emergency landing procedures
(ie, position, oxygen, securing equipment)
• Safety in and around the aircraft, including national aviation rules and regulations pertinent to for medical team members, patient(s), and lay individuals
• Specific capabilities, limitations and safety measures for each aircraft used, which includes specific training for backup or occasionally used aircraft
• Use of emergency locator transmitter (ELT)
• Minimal safety requirements on ground support ambulances used away from base for fixed wing operations, for example, adequate number and functioning seat belts for all team members, no loose equipment
f. Ground operations (RW)
• Landing sites
— On-scene requirements
— Hospital landing site changes or special needs review
• Patient loading and unloading—policy for rapid loading/unloading procedures
• Refueling policy for normal and emergency situations
g. Hazardous materials recognition and response. (Even if not part of the service's mission statement, personnel should be able to recognize a hazardous materials situation if encountered.)
h. Highway scene safety management
i. Survival training/techniques/equipment that is pertinent to the environment/geographic coverage area of the medical service. (Includes water egress survival training* if en-route travels are routinely over large bodies of water such as rivers, lakes, bay areas based on the program risk assessment)
• Smoke in the cockpit/cabin, firefighting in the cockpit/cabin
• Emergency evacuation of crew(s) and patient(s)
Water egress survival training should include: hazards to aircraft and personnel during overwater operations; pre-ditching considerations and procedures; emergency ditching and evacuation procedures; upright emergency evacuation; emergency evacuation; surface water survival; and rescue water skills. Fixed-wing services that are required by Federal Aviation Regulations (FARs) to carry emergency equipment, such as inflatable rafts, must provide this training.
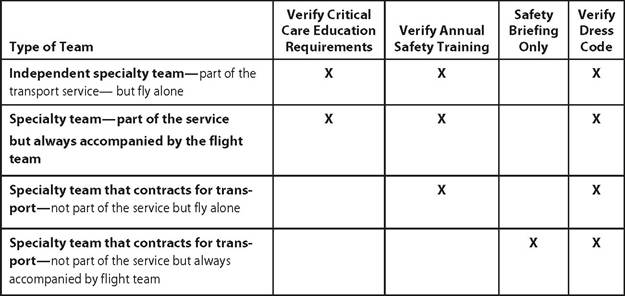
Annual safety training is required to include general aircraft and ambulance safety and emergency procedures unless the specialty team is always accompanied by a regularly scheduled crewmember (see Table 19.1).1
Table 19.1: Safety Training Checklist
More on the topic Frequently Cited Deficiencies Regarding Specialty Teams:
- Frequently Cited Deficiencies Regarding Specialty Teams
- Impact of Specialty Neonatal-Pediatric Transport Teams
- Impact of Specialty Neonatal-Pediatric Transport Teams
- Deficiencies of the lower limb are less frequent than deficiencies of the upper limb, but surgical and rehabilitation management may be more involved.
- Literature Cited
- WORKS AND ARTICLES CITED
- Uncommon Upper-Limb Deficiencies
- Nutritional Deficiencies
- Common Lower-Limb Deficiencies
- Common Upper Limb Deficiencies