Intervention, Prosthetic Treatment, and Adaptive Equipment
Although prosthetic treatment may seem indisputable for an individual with a limb absence or acquired amputation, it is not as straightforward as one might imagine. The inability to provide or restore the function of the human arm and hand poses great challenges to individuals with partial or complete limb loss (77).
These fittings are generally limb-level-dependent as well and vary between passive, body-powered, and externally powered options. Acceptance of prosthesis is a complex issue; factors that influence acceptance include level of limb loss, presence of other complicating medical conditions, comfort and usefulness of the prosthesis, and acceptance of the limb deficiency by the family. In general, the higher the limb absence, the less likely it is that a child will find a prosthesis useful enough to wear it regularly. For example, transradial patients will tend to wear their prostheses more than transhumeral patients, and transhumeral patients will tend to wear their limb more than shoulder disarticulation patients (90).Goals of early intervention and training revolve around achieving age-appropriate milestones. Children with upper limb differences frequently achieve developmental milestones at or around the same age as children without limb anomalies. Prostheses are generally considered around 3 to 6 months of age (91). Until recently, 6 months of age used to be the time at which fitting was initiated (92,93). This was the age chosen because it was the time the child was expected to have achieved sitting balance. Clinical experience versus evidence-based study guides fitting timetables (94). Although there are general guidelines for fittings, the initial fitting is something that is discussed in the clinic between the team members and family. Many children will be fitted with prostheses prior to 1 year of age. Early prosthetic fitting is designed to encourage bimanual tasks, establish a wearing pattern, increase overall independence, provide for symmetrical crawling, and reduce “stump dependence”—sensory dependence on the end of the residual limb (95).
Early fitting does not guarantee acceptance (96). The prostheses needs to fit comfortably, which can be challenging to assess in an infant, be relatively easily donned, equalize lengths with the noninvolved limb, allow for growth, and provide restoration acceptable to family (97).Several different terminal devices may be considered for the first prosthesis. Age-appropriate prostheses are fitted to children; passive prostheses are generally the first design utilized. Options include hands, hooks of various shapes, mitts, and other non-hand designs. The vast majority of parents prefer a terminal device that looks like a hand. For this reason, it is recommended that a passive hand be provided rather than a hook or other non-hand device. The two basic passive hand options for infants are the closed, “crawling hand” design and the open hand design. The parents should be involved in the decision-making process—this involves providing information about the pros and cons of each style and, more importantly, letting the parents decide which design is most acceptable in their eyes. Once the parents accept the child's limb deficiency, they will be more inclined to evaluate prosthetic components based on functional qualities in addition to appearance. If parents are involved in the decision and accept the device, they are more likely to encourage the youngster to wear the prosthesis. Figure 13.7 shows an infant passive hand.
It is questionable whether it is appropriate to fit children with partial hand deficiencies and wrist disarticulations at a very young age. They have long residua and can use them for bimanual tasks. Figure 13.8 illustrates a transcarpal limb deficiency with adequate length for function. The prosthesis would serve the purpose of providing a wearing pattern and also reducing dependence on the sensation of the limb. The
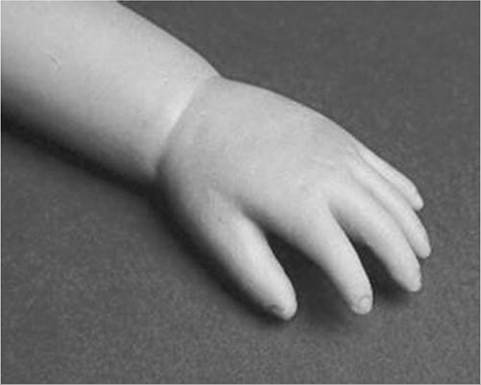
Figure 13.7 RSL Steeper infant foam-filled passive hand.
latter can arguably be considered as a positive rather than a negative. The passive terminal device options can be similar, although there are limitations due to the length available distal to the residuum. Opposition posts are sometimes considered for the child with car- pals and wrist motion. These devices can be rigidly fixed or placed in several different positions to accommodate for grasping different-sized objects.
For the child with a limb that extends distal to the elbow, the initial prosthesis is usually self-suspending, using a supracondylar design, with or without a suspension sleeve. If this is not achievable, a narrow Dacron harness may be designed in a figure-eight configuration. This harness should be easy to put on the child, have elastic as part of the straps for increased shoulder motion, and have snaps or fasteners that make it easy to put on and take off.
The same passive terminal device options are appropriate for the child with a limb deficiency proximal to the elbow. The major difference between these levels is that the absence of the elbow joint makes it more difficult to preposition the terminal device for

Figure 13.8 Transcarpal limb deficiency with adequate length for bimanual tasks.
bimanual tasks. The child is not cognitively ready for an articulating elbow; therefore, a curved shaped “banana” arm is often provided in order for this child to engage the prosthesis with the contralateral hand as well as reach levels that are closer to the midline and face (98). Figure 13.9 displays the passive “banana arm” prosthesis.
The next developmental milestone is walking, which usually occurs at 11 to 13 months of age. This will indicate that the child is ready for a more sophisticated upper-extremity prosthesis. At this time, the child is ready to perform simple grasp-and-release activities using the prosthesis. It is imperative that the family be involved in the clinical decision-making about their child's prosthesis.
The prosthetists should have designed the prosthesis in a manner to accommodate growth. It is best to keep the control system as simple as possible at this early age in order to ensure early success. Other developmental factors to be considered are understanding of holding function, attention span longer than five minutes, and willingness to be handled by an occupational therapist to go through terminal device opening motion.When the child is developmentally ready for terminal device activation, options include body-powered hooks or hands as well as myoelectrically controlled hands. The majority of parents prefer hands; the hands that provide optimal function at this age are myoelec- trically controlled. At this age, the simplicity of control is of paramount importance. An electric hand that is controlled by one electrode in a voluntary opening control scheme has proven effective and natural. This electronic scheme permits the child to activate the hand opening with a contraction (usually on the side of the wrist extensors) and relaxation that enables the hand to automatically close. This electromechanical

Figure 13.9 Transhumeral passive “banana arm” prosthesis.
design is analogous to a split hook, voluntary-opening prosthesis. Designing such an electronic control scheme eliminates the need for the child to maintain muscle contraction in order to continue grasping the object. As the child grows older, another electrode can be added to the flexor side of the forearm, enabling the child to have volitional control opening and closing the myoelectric hand (99).
Myoelectric hands of the past were too large and difficult for a 1- or 2-year-old child to use successfully. Therefore, it was recommended that these hands not be fitted on children until 4 to 5 years of age. Today, it is common for these hands to be fitted successfully on 1-year-old children.
Prosthetic technology has improved dramatically as a result of miniaturization and simpler control to better meet the needs of very young children. Figure 13.10 shows a transradial myoelectric prosthesis with myoelectric hand terminal device.Body-powered devices may not work well for this age group because they lack the requisite force and excursion, as well as the cognitive ability, to relate shoulder motions to terminal device operation. The voluntary-opening-style terminal devices permit the user to grasp an object and allow the force of the elastic bands or springs to keep the object in the terminal device. This may be ineffective if the child cannot overcome the force required to activate the terminal device. The designs of voluntary-opening terminal devices for children are not very aesthetically pleasing, with the exception of the mechanical hands. The hands, however, have the drawback of providing minimal efficiency. Once a cosmetic glove is applied to the mechanical hand, it can lose up to 40% of its efficiency, compared to the function of the hand without the glove voluntary closing terminal devices have gained in popularity, although the child must maintain force and excursion through the harness to maintain grasp on an object. The amount of grasping force is directly proportional to the force that the child puts into the
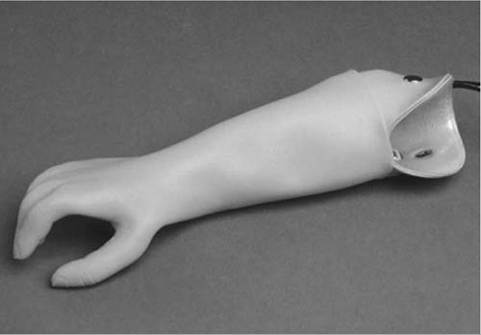
Figure 13.10 Transradial myoelectric prosthesis.
harness (100). The figure-of-eight harness is pictured in Figure 13.11 with straps shown. The prosthetic team can predict the ability of the child to control the myoelectric components when using evaluative tools such as the capacity of myoelectric control (101,102).
By the time children are 4 or 5 years old, they are able to operate virtually all types of prosthetic components and control schemes presently available (100).
The developmental milestones described previously should guide the fitting schedule of the tran- shumeral limb-deficient child.
Because of the nature of a transhumeral prosthesis, it can be more of an encumbrance than the transradial design. This can cause difficulty in rolling over, and may impede the child's development if fitted too early. The terminal device should be activated shortly after the child begins to walk. Terminal devices for the transhumeral level are the same as the transradial. The addition of a prosthetic elbow is the key difference. The first prehensile prosthesis will employ a friction elbow to allow positioning of the terminal device. It is useful to limit the range of motion at the elbow by producing flexion and extension stops to prevent the elbow from flexing excessively during weight bearing activities (eg, crawling). The initial prosthesis may be suspended by a harness or by silicone suction suspension. The silicone suction socket (3S) has proven effective because it allows free range of motion at the shoulder and provides excellent suspension. The child with a transhumeral deficit should be fitted with an activated terminal device once he or she begins to walk.Considerations for terminal device selection include appearance, weight, ease of operation, and cost. The myoelectric hand offers reasonable appearance and ease of operation when controlled by a single-site voluntary opening circuit; however, it is a heavier and more expensive prosthesis compared to body-powered. Either voluntary opening or voluntary closing designs can be used successfully by the transhumeral limbdeficient child once the child has sufficient strength and the cognitive ability to understand how to operate the device. This usually is possible at 2 to 3 years of age. When the child is strong enough to operate an active elbow, usually at age 4 to 5, a conventional body-powered elbow may be provided; however, locking of the elbow by conventional methods may prove challenging. If the child has insufficient strength/ excursion to operate the body-powered elbow, an electric elbow may be considered, although the increased weight may preclude this option. The terminal device illustrated in Figure 13.12 is a voluntary opening split hook and can be utilized on both transhumeral and transradial deficiencies.
The shoulder disarticulation level is treated differently due to the challenge in positioning the shoulder, elbow, and terminal device. The child may be fitted with passive endoskeletal shoulders and elbows with an active terminal device. Current fittings have been utilizing externally powered hands controlled by either electromechanical rocker switches or forcesensing resistors. The child is encouraged to maintain good ranges of shoulder elevation/depression and protraction/retraction in order to make contact with these input devices. The return or enhancement of function using these devices is quite limited. Therefore, there are no “right” philosophies for the fitting of these complicated cases. The team should recognize that prostheses need to be useful to the child in order for him or her to choose to wear them. A useful sport's prosthetic terminal device is illustrated in Figure 13.13.
The phocomelic or bilateral total upper-extremity transverse deficiency patient rarely requires amputation revision; indeed, the terminal digits can activate
Anterior Suspension Strap
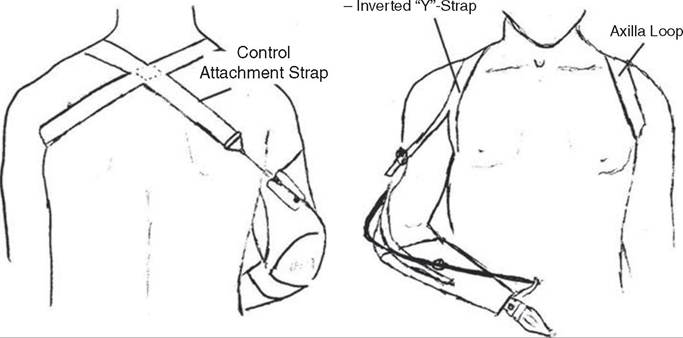
Figure 13.11 Figure-eight harness.
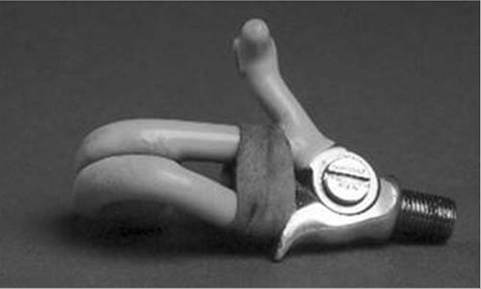
Figure 13.12 Hosmer voluntary opening, split hook terminal device.
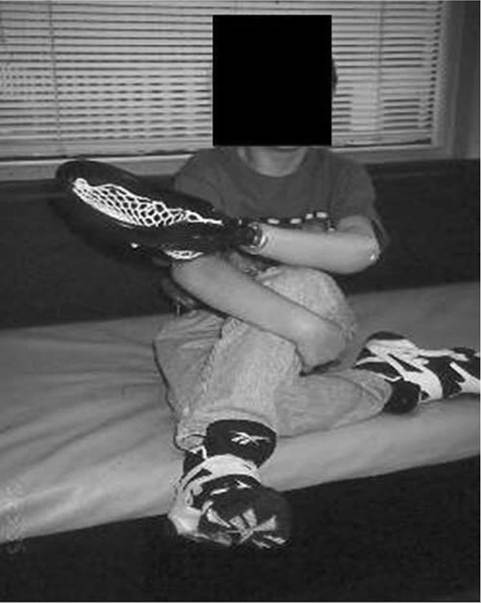
Figure 13.13 Child with TRS High-Fly Fielder terminal device.
switches or myoelectric sensors (90). In the case of higher-level bilateral deficiencies, it is wise to start as simple as possible, recognizing that each child has a certain level of tolerance for “gadgets.” With the vast array of prosthetic components now available, it would be easy for the well-intentioned clinic team to recommend components that would overwhelm the user. Critical factors in the success of the high-level bilateral are prosthetic weight, complexity of control, proprioceptive feedback, wearing comfort components, and motivation and attitude of child and family.