Therapy and Training
The preprosthetic period is mainly focused on the needs of the parents (103). The family level of distress or stress related to the child's limb deficiency will vary (104). It is important during this initial contact for the clinic team to present an honest forecast of the prosthetic plan.
The team members must walk a fine line between presenting the prosthetic options in an honest manner without sounding negative or disheartening. After all, prosthetic technology with all of its sophistication is still far from the ideal of replacing a physiological arm.The parents should be encouraged to treat the child as they would a child with normal limbs. Many parents benefit from being introduced to other parents and children with similar limb deficiencies (106).
Typically, children younger than 3 years of age have therapy provided in the home. Prone positioning is important for encouraging trunk extension and mobility. Gross motor milestones are generally not delayed, but may be affected by asymmetry imposed by unilateral upper limb deficiencies. Children compensate and substitute for the missing action of limbs. Therapists bridge the delivery of the prosthesis to the initiation of function and create a comfortable environment for children to explore options, with or without the prosthesis. The goal is to increase the child's awareness of the affected side, including the prosthetic device. The child should also be encouraged to use the prosthesis for transitional movements, such as sitting to crawling, and leaning on the prosthesis for weight bearing while reaching with the dominant hand. The parent is encouraged to maintain telephone contact with the therapist to answer questions regarding follow-through with prosthetic usage. A recheck through the clinic should be scheduled within a month after delivery of the prosthesis and then every three to four months.
When the terminal device is activated, the therapist will again provide initial instruction to the parents and child. A structured approach to use of the terminal device assists parents, child, and therapist in gaining confidence and competence (106). The therapist will work with the child and parents using toys that encourage bimanual use, such as Lego bricks, pop beads, and stringing beads. Initially, it is useful to concentrate on activities that require the prosthetic side to hold while the dominant hand manipulates. When training a child in the use of a myoelectric hand using this control scheme, the therapist should encourage activities that cause the hand to open. Because of the placement of the electrode over the forearm extensors, activities that elicit an extensor activity are appropriate. Once the hand is open, the therapist can quickly place a toy in the hand and encourage the child to release it. The child will learn through repetition.
It is unrealistic and inappropriate to teach the child to use the prosthesis for dominant hand activities. Children with high-level bilateral upper- extremity limb deficiencies will utilize their feet in a natural manner. Assistance is necessary for donning and doffing pros- theses. The child with an isolated limb deficiency or amputation is capable of achieving age-level academic skills. Few studies have been done to define achievement academically. Good social adjustment is reported for children with myoelectric prosthetic users (107). School placement is almost entirely within the regular school system, with an Individual Education Program (IEP) to address educationally related function. Occupational therapists will assist with issues of grasp and fine motor control for paper, computer, and ADL tasks needed in school. Informational pamphlets have been developed for the teacher to prepare the able-bodied students for integration of children with physical disabilities into the regular education classroom.
Adapted physical education may be necessary, but regular physical education is often sufficient. The philosophy promoted for children with physical disability is that of “participation, not observation.” Participation in athletic endeavors such as skiing, tennis, and other more mundane exercise improves the self-concept of the child or adult with limb deficiency. Specialized, adaptive prosthetic components that enable unilateral or bilateral handless persons to participate in sports such as golf, shooting, and ball sports have escalated since the 1980s.
Functional assessments recently developed to determine the use of upper-extremity prosthetics and function have included Assisting Hand Assessment, the Prosthetic Upper Limb Functional Index, The University New Brunswick Test of Prosthetic Function, Child Amputee Prosthetic Project-Functional Status Index, Child Amputee Prosthetic Project-Functional Status Index Preschool, Shriners Hospital Upper Extremity Evaluation (SHUEE), Capacity for Myoelectric Control (101), and Unilateral Below Elbow Test (108-114). It is typical for children to perform activities of daily living with their prosthesis, but often choose not to utilize them (115). In addition, prosthetics are often utilized for specific tasks versus everyday tasks. Children typically utilize nonprosthetic options ages 3.5 through 13 years of age (103).
Outcomes related to patient satisfaction are increasingly important to evaluate for prosthetics (116,117).
Recent studies have indicated that children with unilateral, below-elbow deficiencies who do not wear prostheses perform as well or better than their counterparts who wear prostheses (77).
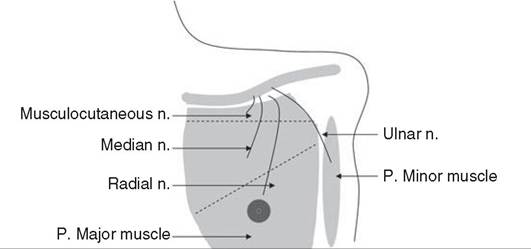
Figure 13.14 Proposed nerve transfer for targeted muscle reinnervation of an individual with shoulder disarticulation amputation.
More on the topic Therapy and Training:
- Leadership Training in Military Legitimacy
- Current Education and Training Requirements
- Legal Education and Training Review
- Training
- Training
- PARENTERAL FLUID THERAPY
- Training for Survival and Emergency Conditions
- Training for Survival and Emergency Conditions
- Training
- Physical and Occupational Therapy
- Training Strategies
- Training Strategies
- Personnel and Training
- Personnel and Training
- Training Opportunities
- Training Opportunities