INTRAUTERINE INFECTIONS
Term intrauterine (IU) infections denotes in utero fetal infection, either transplacentally or as an ascending infection from maternal birth canal.
IU infections are the commonest cause of fetal loss (abortions/stillbirths), congenital malformations and intrauterine growth retardation (IUGR) in India.
While infection in first trimester usually results in fetal loss or congenital malformations, later infections cause IUGR. Etiology: IU infections are usually viral, though may also be caused by many bacterial, protozoan and spirochetal agents (Table 12.47). In clinical practice, common IU infections are popularly referred with an acronym TORCH—Toxoplasma Gondi, Others, Rubella, Cytomegalovirus disease (CMV) and Herpes simplex infections.Clinical presentation: Live born babies with IU infections usually present with following features at birth (Table 12.48), though some manifestations may develop or diagnosed at a later age.
• History of maternal illnesses, e.g. fever, rashes, lymphadenopathy, jaundice and vaginal lesions
TABLE 12.47: Common intrauterine infections
| a. | Viral | Rubella, CMV, HSV, HBV, HIV Varicella, mumps, parvovirus B19 |
| b. | Bacterial | Tuberculosis, gonococci gram-ve organisms, listeriosis |
| c. | Spirochetal | Syphilis |
| d. | Protozoal | Toxoplasmosis, malaria |
| e. | Others | Mycoplasma, chlamydia |
TABLE 12.48: Clinical indicators of intrauterine infections
• History of maternal infection
• Intrauterine growth retardation (IUGR/LBW)
• Hepatosplenomegaly and/or Jaundice
• Purpura
• CNS: Microcephaly, hydrocephalus, mental retardation
• Ocular: Microphthalmia, cataract, chorioretinitis
• Hearing impairment
• Congenital malformations, e.g.
CHDs• Others: Skin rash/vesicles, pneumonia, etc.
during pregnancy is present in gt;50% cases, though missed frequently.
• Low birth weight (IUGR) is the commonest manifestation in 60-70% babies. However, babies with congenital syphilis tend to be large-sized due to hydrops fetalis.
• Hepatosplenomegaly is present in 50-60% cases, with/without evidence of active liver disease. Neonatal jaundice is common in Toxoplasmosis and CMV infection.
• Purpuric lesions due to thrombocytopenia are common in CMV and congenital rubella, though serious internal bleeds are rare.
• Meningoencephalitis, is usually sub-acute and presents with microcephaly (rubella or CMV), hydrocephalus (toxoplasmosis) intracranial calcifications (CMV, rubella), mental retardation and seizure disorders. Intracranial calcifications are typically periventricular in CMV and diffusely nodular in toxoplasmosis.
• Ocular abnormalities: Extrinsic abnormalities, e.g. micropthalmia, microcornea, corneal opacities and cataracts are more common in congenital rubella. Presence of uveitis or interstitial keratitis indicates CMV and congenital syphilis respectively. Chorioretinitis is present in many infections and typically central in toxoplasmosis, peripheral with normal macula in CMV and salt-pepper type in rubella infections. Chronic retinopathy may leads to optic atrophy, strabisumus and searching nystagmus in older children.
• Hearing impairment is common in congenital rubella and CMV infections.
• Congenital heart, diseases are common in congenital rubella, specially PDA or sub-valvular PS.
• Other manifestations include skin vesicles in herpes simplex, rash or snuffles in congenital syphilis, pneumonia and neonatal septicemia.
Diagnosis of IU infections depends on:
• Presence of clinical indicators (Table 12.48) or antenatal history suggestive of maternal infection.
• Non-specific cord IgM levels of gt;20 mg/dl indicate possibility of IU infection and may be used as a screening test.
However, it has no differentiating value between various causes.• Specific serology (TORCH screen) for organism specific IgG and IgM antibodies. Single IgG titers are unreliable due to passive transplacental transfer from mother. IgM titers are more reliable and indicate actual fetal infection.
• Serodiagnosis of any IU infection requires positive IgM titers or IgG titers multi-fold higher than maternal values or rising IgG values after 3-4 weeks.
• Isolation of specific etiological agent by microbiology or PCR testing is confirmatory, though rarely possible.
• Relevant investigations: X-ray skull and long bones, e.g. knee are indicated in all cases to detect, e.g. intracranial infections (CMV, toxoplasmosis), osteochondritis, periosteal reaction, and metaphysitis in long bones (congenital syphilis), longitudinal linear radiolucent areas with increased bone density (congenital rubella).
D/D of common IU infections is given in Table 12.49, while some are discussed in detail, as follows.
Congenital rubella syndrome (CRS) is consequence of rubella infection in previous non-immune pregnant mothers, which produces mild viral illness in pregnant mothers, but with devastating effect on fetus. For acquired infection, see Ch 10.18.
Mode of infection: Fetal infection is acquired trans- placentally and risk of transmission is highest (~90%) when mother is infected in first trimester. Infection beyond 20th week is rarely associated with CRS, except sensory-neural deafness.
Clinical features of CRS include—(a) IUGR, (b) neurological signs, e.g. microcephaly and mental retardation, (c) ocular signs, e.g. congenital cataract, microphthalmia, microcornea, salt-pepper retinopathy, etc., (d) sensorineural hearing loss, (e) hepato- splenomegaly with/without jaundice, (f) anemia and thrombocytopenic purpura and (g) congenital heart diseases, specially PDA or subvalvular PS (Fig. 12.20).
Diagnosis usually rests on specific serology, i.e. (a) elevated IgM titers in cord/neonatal blood, or (b) gt;4- fold higher IgG titers in newborn than in mother, or
(b) rising IgG titers after one month.
Viral isolation from nasopharynx or urine is confirmatory, but rarely feasible. Management: Prevention of CRS revolves around prevention of maternal infection during pregnancy by (a) MMR immunization in childhood or unimmunized women in reproductive age, (conception should be avoided at least 3 months after immunization), or (b) avoidance of contact with suspected case during pregnancy, including a case of CRS (as virus may be shed up to 1 year).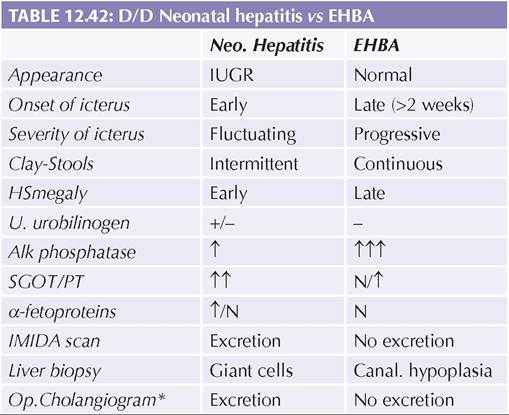
Fig. 12.20: Congenital Rubella Syndrome: (A) Microphthalmia with microcornia (Inset: Corneal opacity); (B) Celery-stalk appearance on X-ray knee.
TABLE 12.49: Comparative features of important intrauterine (TORCH) infections

TP: Transplacental infection, PP: Peripartum infection during vaginal delivery, BM: Infection via breast milk, *in primary infection during pregnancy, lt; 1% in recurrent infection. ** See text for details
Accidentally exposed and unimmunized pregnant mothers should be screened serologically, immediately and after 4 weeks of exposure. Risk of CRS is negligible in seropositive mothers at the time of exposure. However, those who seroconvert after exposure have maximum risk of CRS and should be counselled accordingly. If abortion is not an option, immunoglobulin prophylaxis is advisable immediately after exposure, to reduce risk of CRS.
Cytomegalovirus disease: Neonatal CMV infection is a consequence of primary maternal infection during pregnancy with risk of transmission being ~40%. Maternal reinfection or reactivation of previous infection is unlikely to produce neonatal disease. For acquired infection, see Ch 10.24.3.
Mode of infection: Neonatal CMV infection may occur: (a) in utero during maternal viremia after primary infection in pregnancy, (b) during delivery, by the virus present in genital passage, or (c) post-natally by infected breast milk or blood products.
Maternal infection in12
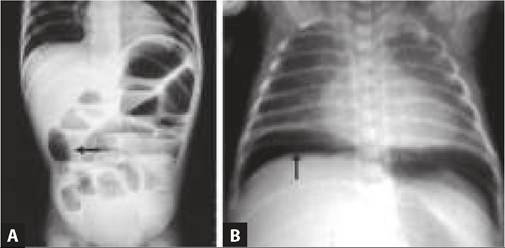
Fig. 12.21: Periventricular calcification in congenital CMV infection.

Fig. 12.22: Diffuse intracranial calcifications and lesions in toxoplasmosis.
early pregnancy is usually associated with more severe fetal disease.
Clinical manifestations depend on timing of infection and divided into three categories:
a. Asymptomatic infection, but with late developmental abnormalities (15%), e.g. deafness, mental retardation, spasticity and microcephaly.
b. Symptomatic but not life-threatening infection, with - (a) IUGR, (b) neurological signs, e.g. microcephaly, intracranial periventricular calcification (Fig. 12.21), hearing deficit, mental retardation, etc., and (c) ocular signs, e.g. peripheral chorioretinitis without macular involvement.
c. Acute sepsis-like manifestations with—(i) hepato- splenomegaly, (ii) thrombocytopenic purpura, (iii) severe jaundice, and (iv) pneumonitis.
Diagnosis usually rests on serology though definitive diagnosis is possible by virus isolation or PCR testing in urine or saliva.
Treatment: IV Ganciclovir (6 mg/kg/dose q12hr) or PO Valganciclovir (16 mg/kg/dose q12hr) for 20 days is the drug of choice for acute manifestations, e.g. preumonitis or chorioretinitis, along with standard/hyperimmune IVIG (500 mg/kg/alternate day 10 doses). However, its utility in CNS disease is not established. Foscarnet is another alternative, under evaluation.
Congenital toxoplasmosis is a consequence of maternal infection during pregnancy, specially in last trimester. Fetal infection due to pre-pregnancy infection is extremely rare.
Mode of infection: Fetal infection is acquired trans- placentally, with risk of transmission being ~60% in last trimester infection, ~3-4 times higher than in first trimester infection.
Clinically, congenital toxoplasmosis may present with: (a) prematurity and IUGR, (b) neonatal disease with anemia, purpura, jaundice, and neurological disease, or (c) neuro-ocular sequelae of untreated infections in later life.
Characteristic features include—(a) neurological disease with hydrocephalus, diffuse intracranial calcifications (Fig. 12.22) and seizures; or (b) ocular disease with central choreoretinitis and secondary optic atrophy.
Diagnosis usually rests on elevated Toxo-IgM levels, though presence of tachyzoites in placenta on immuno- fluorescent staining) or positive CSF-PCR is confirmatory. Treatment is of limited value in severely affected newborns, as the damage has already occurred. It should begin as early as possible and includes:
• Severe disease are treated with PO Pyrimethamine (1 mg/kg/day for 6 months than 0.5 mg/kg/day for next 6 months) and Sulfadiazine (100 mg/kg/day for 12 months, along with Folinic acid 10 mg alternate days. Steroids are indicated for 8-12 weeks in cases with acute inflammatory injury, e.g. chorioretinitis or elevated CSF protein gt; 1 gm.
• Mild or subclinical cases born to a mother with definite primary infection may be treated less intensive regimens for shorter duration.
Prevention involves treatment of maternal infection during pregnancy with PO Spiromycin (2 gm/day) from 20th week onwards, along with Sulfadiazine (75 mg/kg/ day) and Pyrimethamine (25 mg BD for 2 days, than OD for 7 days than biweekly). Folinic acid (5 mg bi-weekly) should be given with Pyrimethamine to prevent folic acid deficiency.
Congenital syphilis is a rarity in recent years due to early recognition and treatment of maternal disease.
Mode of infection: Congenital syphilis is usually acquired as transplacental infection during spirochetemia in mother, or rarely at the time of delivery through infected
TABLE 12.50: Late clinical stigmata of congenital syphilis
Bony changes (due to chronic periosteitis)
• Frontal bossing
• Olympian brow (prominent forehead)
• Saddle nose (depressed nasal bridge)
• Perforated nasal septum (due to snuffles)
• Higoumenaki's sign (thick sternoclavicular joints)
• Saber shins (anterior bowing of Tibia)
• Scaphoid scapula (convex medial border)
Dental abnormalities (manifests ~6 years of age)
• Hutchinson teeth (barrel-shape upper incisors)
• Notched teeth with abnormal enamel and severe caries
• Mulberry molars (multi-cuspid lower first-molars)
Residual mucocutaneous lesions
• Rhagades (Spoke-like perioral/perianal scars)
Hypersensitivity manifestations
• Interstitial keratitis with/out corneal opacities
• Clutton joints* (painless joint swellings) *due to intermittent syonovitis, specially at knee
birth canal. Infection is usually transmitted in last trimester, though spirochetes may cross placenta at any stage.
Risk of transmission is highest (~100%) in mothers with recent infection, decreases gradually and unlikely after 5 years of maternal infection.
Clinical manifestations: Early trimester infections often lead to abortions, stillbirths (40%) or hydrops fetalis due to severe anemia, while late trimester infections are often associated with large placenta and present as follows (IUGR is rare).
a. Early manifestations during first 2 years of life, are analogous to secondary syphilis, including Failure to thrive, generalized erythematous rash, Nasal snuffles, painful and restricted limb movements (pseudoparalysis), hepatosplenomegaly and pan/ bicytopenia. Pneumonia and meningitis may be present.
b. Late manifestations (stigmata) after 5-10 years, due to chronic inflammatory changes in skin, bones and teeth, or hypersensitivity (Table 12.50).
Diagnosis may be confirmed by dark field microscopy, FTS-ABS IgM or serial VDRL with rising titers after one week. A single VDRL titer gt;4 times of the mother or Positive VDRL in CSF may also be considered as diagnostic. VDRL may be false-positive in babies of infected mothers due to transplacental transfer of antibodies. X-ray knee joint may be diagnostic in a suspected case, showing periostitis and osteochondritis at the ends of long bones (Fig. 12.23).
CSF examination is indicated in all cases for biochemistry and VDRL test, as longer penicillin therapy is required in cases with CNS involvement. However, CNS involvement is possible without CSF abnormalities. Treatment of a baby born to VDRL positive mother depends on anticipated risk of infection. Adequate
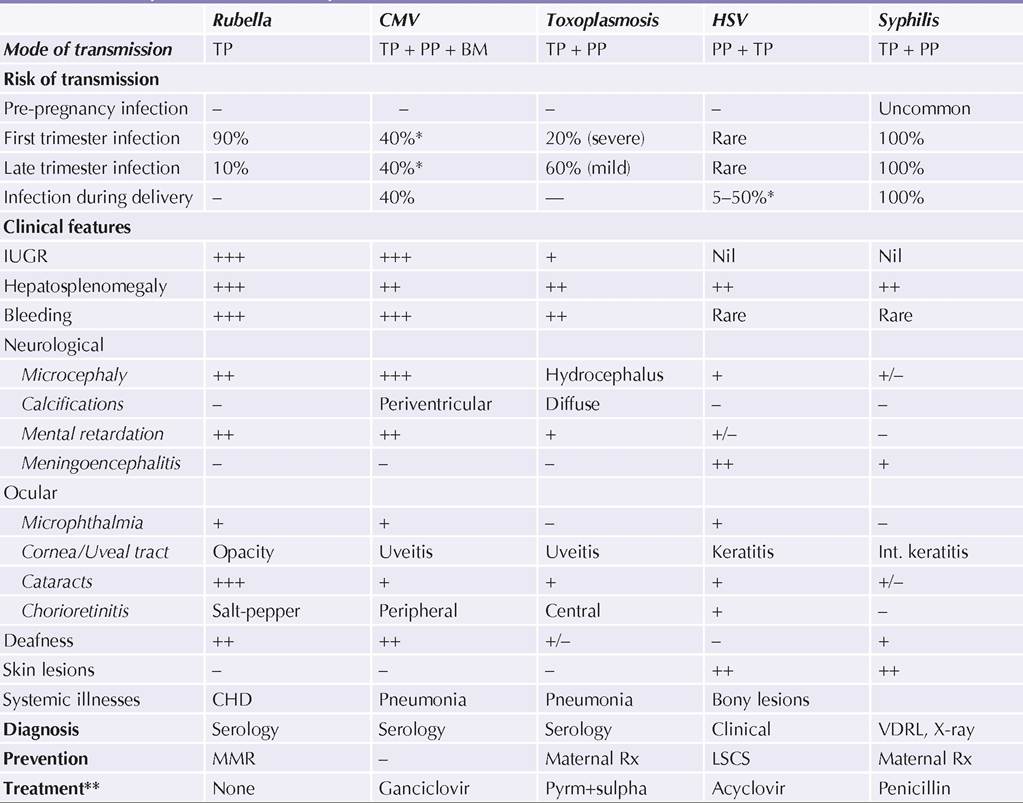
Fig. 12.23: Congenital syphilis : Periosteitis and osteochondritis at the ends of long bones.
maternal therapy, if received at least 30 days prior to delivery, virtually eliminates the risk of transmission.
All other cases must be treated either with IV Crystalline Penicillin G (50,000 lU/kg/dose 8-12 hourly) or IM Procaine penicillin (50,000 lU/kg once a day) for 10-14 days. Longer therapy (3 weeks) is necessary in cases with CNS involvement.
Perinatal HSV infection is a consequence of primary or re-activation HSV infection in mother with active disease during pregnancy. For acquired infection, see Chapter 10.24.1.
Mode of infection: HSV infection is usually acquired during delivery through infected birth canal (peripartum). Rarely, baby may be infected in utero (lt;5%) or as postnatal nosocomial infection.
Clinically, peripartum infection presents with signs of active disease, e.g. typical skin/mucosal lesions (grouped vesicles), meningitis and respiratory distress during 1st week. However, early in utero infection may present with sequelae, e.g. microcephaly, microphthalmia, chorioretinitis and old skin scars (suggestive of in utero vesicles).
Diagnosis is largely clinical but may be confirmed by the viral culture or PCR from urine or saliva in first two weeks of illness. Tzanck cells are also present in vesicular scrapping.
Treatment: Acyclovir therapy (IV 20 mg/kg/dose TDS for 14-21 days) is the mainstay of treatment in perinatal HSV infection, apart from supportive and symptomatic care.
Prevention: Obstetrical care in mother with genital HSV includes—(a) elective LSCS to avoid vaginal passage, (b) Viral cultures from eyes, nose, mouth, urine and stools of baby at 48 hours, and (c) prophylactics acyclovir therapy to baby, if mother is symptomatic at the time of delivery.
Some other important intrauterine infections, e.g. congenital tuberculosis, congenital malaria and perinatal HIV infection have been discussed in respective chapters.
More on the topic INTRAUTERINE INFECTIONS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- HEPATOMEGALY
- Genitourinary Infections
- HERPETIC VIRAL INFECTIONS
- INTRODUCTION
- INTRACRANIAL INFECTIONS
- Malassezia spp. Infection: Malasseziasis
- NEURAL TUBE DEFECTS
- CYTOMEGALOVIRUS DISEASE____
- ACTINOBACILLUS INFECTIONS