Leg Length Inequality
Leg length inequality is common, with estimates of up to one-third having a 2-cm or less discrepancy measured between the length of their legs (6,303). There are two basic types of leg length discrepancies: true and apparent.
True leg length discrepancy is present when bilateral leg length measurements between the greater trochanter and the medial malleolus demonstrate shortening on one side. Apparent leg length discrepancies are present when bony lengths are the same but joint alignment or pelvic femoral asymmetry is present (eg, adductor spasticity, pelvic obliquity). Apparent discrepancies can best be measured using a tape measure from the umbilicus to the medial malleolus of either side.Radiographic measurement is the most reliable. The scanogram technique avoids magnification by taking separate exposures of the hip, knee, and ankle so that the central x-ray beam passes through the joints, giving true readings from scale (Fig. 14.23) (304,305). CT scanogram is still the standard, reducing errors from angular deformity (306). If the examination is done specifically for this purpose, economic cost can be competitive (multiple sections unnecessary) and radiation exposure less with microdose technique (307,308). Causes of true leg length discrepancy are many and can be classified by growth retardation versus growth stimulation (6,20). Growth retardation has included conditions such as congenital hemiatrophy, developmental hip dysplasia, Legg-Calve'-Perthes disease, slipped femoral capital epiphyses, polio, achondroplasia and dyschondroplasia, and severe burns. Causes by growth stimulation include congenital giantism, Wilm's tumor vascular abnormalities such as Klippel- Trenaunay-Weber, thrombosis or femoral or iliac veins,
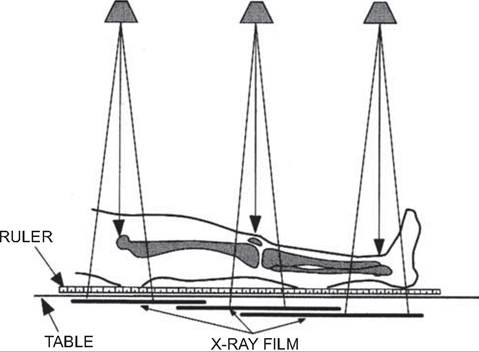
Figure 14.23 The scanogram technique avoids errors of magnification and is preferred for children who can remain still for three exposures.
and traumatic arterial venous aneurysms. Tumors such as giant cell, neurofibromatosis, and bony fractures can cause other growth retardation or growth stimulation. The child with true hemihypertrophy needs to be screened every four months for the possibility of Wilm’s tumor (6,309) up through the age of 8 and every 6 to 12 months through the age of 10. Eighty percent of Wilm’s tumors present prior to the age of 8, with an average age at presentation of 3 years. The tumor may be associated also with aniridia (lack of an iris in the eye) and secondary metastases to the skeleton. A firm, nontender abdominal mass may be palpated. Damage to the growth plate with trauma and epiphysiodesis, including fractures with marked-over riding of fragments, tend to cause more growth retardation.
Treatment objectives include obtaining leg length equality, producing a level pelvis, and improving function. Leg length discrepancy of less than 1.5 cm is usually just observed. Shoe lifts can be utilized for differences up to 3 cm. Horizontal alignment of the iliac crest or sacral base in the standing position should also be witnessed with appropriate shoe lifts in place. Early attention should be given by the age of 7 or 8 to observe and record the pattern of growth and appropriately time the growth plate arrest.
The Greulich-Pyle norms for skeletal maturation of the hand (310) and the charts of Green-Anderson (311) are used for prediction of future growth and the timing of surgery when stapling epiphysiodesis of the longer side is considered for true discrepancies between 3 and 6 cm. Stapling techniques across the physis produce a tethering effect and can be removed later once equalization has been achieved (312,313). Surgical epiphysi- odesis is an all-or-nothing procedure that completely and permanently arrests physeal growth. The principle is to produce a symmetrical bony bridge that tethers the physes and prevents future growth (314). Epiphysiodesis is most commonly performed two to three years prior to maturity (girls age 11 or 12 years; boys age 12 or 13 years).
Shortening procedures can also include removal of a section of bone for limb equalization performed in adults or adolescents who are no longer growing (11).
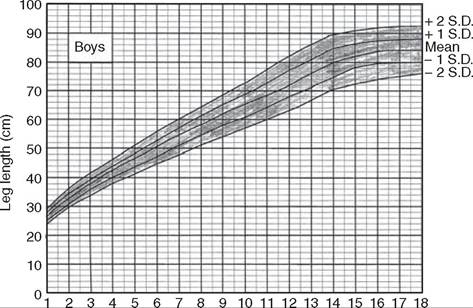
Charts of Green and Anderson are displayed in Figures 14.24 and 14.25, respectively. Total leg length versus skeletalage for boys and girls are shown respectively. Plotting of leg length versus skeletal age is critical in the timing of any surgical procedure projecting limb length equalization into the future (315,316). The Green and Anderson studies provide good documentation for the general population studied, but no guarantees for children of other races or genetic stock. Additional and more specific determination of leg length discrepancy can be obtained through three additional methodologies (6,11). These include the arithmetic method, the growth remaining method, and the straight line graph method—not described further, as such is beyond the scope of this text. Growth discrepancies beyond 6 cm are best treated by limb lengthening through such methods as Wagner or Ilizarov (6,11). Unlike epiphysiodesis, leg-lengthening procedures can be performed at almost any skeletal or chronologic age. Discrepancy greater than 15 to 20 cm should consider combined shortening and lengthening procedures in addition to amputation. Codivilla first reported mechanical bone lengthening in 1905 (317). Subsequent advancement in limb lengthening has been by the method of Ilizarov (318), whose biologic principle of distraction osteogenesis has revolutionized the surgery. Ilizarov’s circular external fixation system is complex, but provides for multilevel correction, including angular deformities and lengthening simultaneously (Fig. 14.26). Corticotomy technique is utilized with care so as not to disturb the medullary cavity contents so that they may make their greatest contribution to osteogenesis during lengthening (6,11).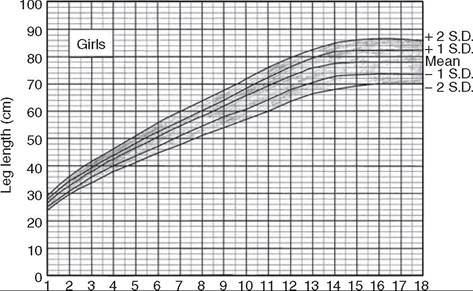
Skeletal age (year)
Figure 14.24 Grafts showing total leg length vs. skeletal age for girls. It provides useful analysis of leg length data, allowing a projection into the future on the basis of present status.
Skeletal age (year)
Figure 14.25 Grafts showing total leg length vs. skeletal age for boys. It provides useful analysis of leg length data, allowing a projection into the future on the basis of present status.
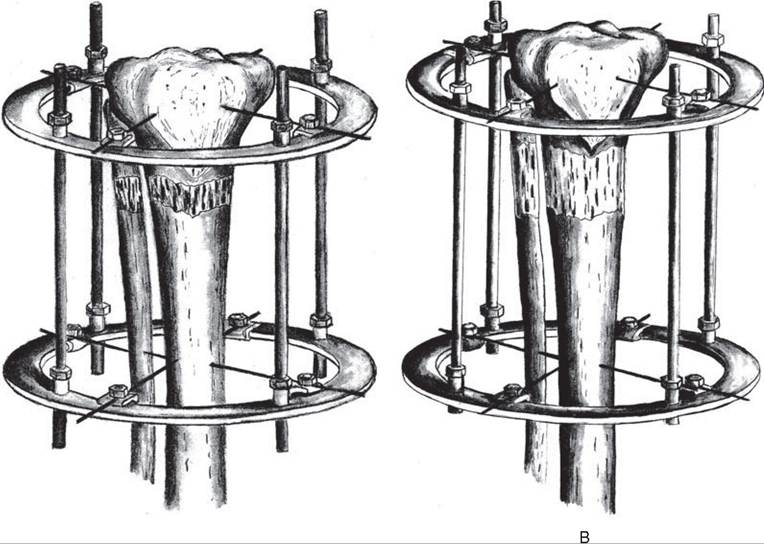
Figure 14.26
(A) Sequential metaphyseal lengthening. (B) Elongation through the active metaphysis promotes osteogenesis and strength by the large crosssectional area across the lengthening gap.
A
Elongation through the metaphyses promotes osteogenesis because metaphyseal bone is so active and promotes strength by the large cross-sectional area. The lengthening process begins approximately 5 to 10 days after surgery. Lengthening of 1 mm per day or approximately 1 inch per month is recommended (6,11). External fixators are worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. A normal lifestyle during treatment is encouraged. Some children even go swimming with the external fixator in place. Complications include pin tract infections (most common), fracture, axis deviation, delayed union, and soft tissue contractures. A child whose family is not capable of sustained follow-up may be a poor candidate for limb lengthening. Significant patient and family education needs to occur, including preoperative and postoperative phases, preparing the child and family both physically and emotionally for the long treatment. Counseling services may prove helpful. Rehabilitation services are most helpful, including frequent physical therapy visits for any successful long-term outcome.