NUTRITIONAL ASSESSMENT
Nutritional assessment is a vital component of child health examination, not only to detect early undernutrition but also to plan appropriate counseling and interventional strategies.
While often used interchangeably, term nutritional assessment and dietary assessment have different connotations.Dietary assessment denotes assessment of actual dietary intake by the child as compared to recommended dietary allowances for the age and gender to identify the deficit/s, if any.
Nutritional assessment is a broader term to encompass dietary assessment as well as assessment of the nutritional status in terms of anthropometric, clinical and biochemical parameters to identify presence of clinical or subclinical nutritional deficiencies, which may or may not be due to dietary causes.
Nutritional assessment is a comprehensive process, involving:
• Dietary assessment, generally based on the 24-hours dietary-recall method. Other methods of dietary assessment, e.g. diary method or replicate diet are rarely used in clinical practice.
• Anthropometric assessment by recording body measurements, e.g. weight, height and mid-upper arm circumference and comparing them with age/ gender related norms to identify growth delay, the most common consequence of nutritional deficiencies.
• Clinical assessment for signs of macronutrient or micronutrient deficiencies.
• Biochemical assessment in selected cases to confirm presence of suspected nutrient deficiencies.
A. Dietary assessment: Dietary history must be relevant to the age, though basic information about early infant feeding (breast/top feeding) and complimentary feeding should be recorded in all cases. Important aspects of dietary history are as follows:
• In infants lt; 6 months, dietary history must concentrate on the type of feeding, e.g. breast/top feeding, appropriateness of breastfeeding practices, problems encountered during breastfeeding, reasons for initiating top-feeding, appropriateness of top feeding, if practiced.
• In children from 6 months-2 years, dietary history must focus on complimentary feeding along with a quick review of early infant feeding, with special emphasis on age of introducing complementary feeds, adequacy of these feeds in terms of quality (minimum dietary diversity) and quantity (minimum meal frequency), and problems encountered during complementary feeding. It should also record whether the breastfeeding has been continued.
• In children gt; 2 years, dietary history should concentrate on the current food intake apart from quick review of the early infant feeding and complementary feeding.
In clinical practice, dietary intake is usually calculated by dietary recall method, by:
• Asking the mother to recall daily consumption of different food items during last few days before the onset of present illness,
• Calculating the average daily intake of nutrients, mainly energy and proteins using known nutritional value of common Indian feeds (Tables 5.9 and 5.10), and
• Then comparing this calculated intake with reference nutritional requirements for the chronological age, (Table 5.1), to find out the deficit/s, if any.
Other methods to assess dietary intake, e.g. diary method or replicate diet method are used only for research purpose.
B. Anthropometric assessment: Three anthropometric indices are commonly used for regular nutritional assessment-weight, length/height and mid upper-arm circumference or MUAC (in children lt; 5 years), which should then be compared with age-related reference values (Ch 2.5).
Age-independent parameters, e.g. are useful when the exact chronological age of child is in doubt. These
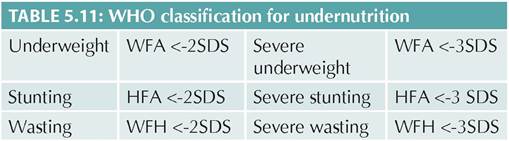
WFA: Weight for age; HFA: Height for age; WFH: Weight for height; SDS: Standard deviation score
parameters are derived by comparing the relationship between two age-related parameters—one early indicator, e.g. weight and other late indicator, e.g.
height. Weightfor height is the commonly used age-independent indicator of undernutrition.While weight is an early indicator of nutritional faltering (wasting), height is not be affected for many months and hence considered as an indicator of longterm nutritional deprivation (stunting). Based on anthropometric data, child may be classified as normal, wasted, stunted or wasted and stunted, with different grades of severity as per WHO classification (Table 5.11).
Screening tests are simple, inexpensive tools used in large nutritional surveys of pre-school children, usually based on MUAC, which is fairly consistent between 1-5 years of age. Commonly used screening test include:
• Shakir's tape, a special plastic tape with three color zones-green, yellow and red, each representing MUAC of gt;13.5 cm, 12.5-13.5 cm, and lt;12.5 cm respectively. When applied on the mid-arm, green zone indicates normal nutrition, yellow zone warns borderline PEM and red zone indicates severe malnutrition.
• Bangle test uses a bangle with inner diameter of 4 cm. When slipped over the forearm, if it crosses the elbow, malnutrition is present.
C. Clinical assessment involves thorough physical examination and search for warning signs for nutritional deficiencies, if present. While it is the simplest method to search for nutritional deficiencies, drawbacks include: (a) sub-clinical deficiencies can be missed, (b) quantification of the severity may be difficult, and (c) nutritional deficiencies with common clinical presentations may not be precisely identified, e.g. xerosis may be due to vitamin A or essential fatty acid deficiency, or pallor may be due to iron or folic acid deficiency.
D. Biochemical assessment is indicated only in selected cases to confirm the presence of selective nutrient deficiency or to identify subclinical deficiencies, if necessary for the purpose of early diagnosis and treatment. Relevant biochemical tests to detect subclinical nutritional deficiencies have been discussed in respective chapters (Ch 6.1-6.7).
BIBLIOGRAPHY
1. ICMR—National institute of nutrition. Nutritional requirements for Indians. ICMR. 2020.
2. Chandrakal BS et al. Difficulties in BF standard treatment guidelines. Indian Academy of Pediatrics. 2022.
3. Breastfeeding Promotion Network of India. Management of breastfeeding. [online] Available from http://www.bpni. org/docments/Management-of-BreastFeeding.pdf. [Last accessed December, 2021].
4. World Health Organization: Baby Friendly Hospital Initiative: Revised, Updated and Expanded for Integrated Care. WHO and UNICEF, 2009. Available at: http://www. who.int/Hyderabad, 2011.
5. Tiwari S et al. Infant and young child feeding guidelines, 2016. Indian Pediatr. 2016; 53(8):703-13.
6. Bharadva K et al. Prevention of Micronutrient Deficiencies in Young Children: Consensus Statement from Infant and Young Child Feeding Chapter of Indian Academy of Pediatrics. Indian Pediatr. 2019;56:577
7. Gupta P et al. IAP guidelines on fast and junk foods, sugar sweetened beverages, fruit juices, and energy drinks. Indian Pediatr. 2019;56:849.
8. National Institute of Nutrition. Dietary guidelines for Indians- A manual. National Institute of Nutrition, Hyderabad, 2011.
More on the topic NUTRITIONAL ASSESSMENT:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- 4 Preconception Counseling and Prenatal Care
- REVIEW OF FORENSIC ASSESSMENT INSTRUMENTS
- FIVE COMPONENTS OF LEGAL COMPETENCIES