Serum Laboratory Studies
Those neuromuscular diseases with inherent sar- colemmal muscle membrane injury often show significant elevations in transaminases, aldolase, and creatine kinase (CK). The CK enzyme catalyzes the release of high-energy phosphates from creatine phosphate.
It occurs mainly in muscle and leaks into the serum in large amounts in any disorder involving muscle fiber injury. The MM fraction is specific to skeletal muscle. The CK value may be significantly elevated in early stages of DMD and BMD, with values up to 50-100 times normal. A normal CK value may help exclude DMD and BMD. Overlap in CK values occurs between DMD and BMD. Other forms of muscular dystrophy, such as Emery-Dreifuss muscular dystrophy (EMD), LGMD, FSHD, and congenital muscular dystrophy, may show moderate elevations in CK. However, in congenital muscular dystrophy, the CK value may be extremely variable, ranging from normal values to a fairly marked elevation. There is no close association between disease severity and CK values. In all dystrophic myopathies, the CK values tend to decrease over time, with increasing severity of the disease owing to progressive loss of muscle fiber and irreversible cell death. Thus, a 3-year-old with DMD may have a CK value of 25,000, while a 10-year-old with DMD may show a CK value of 2,000. Other conditions with significant elevations in CK may include polymyositis, dermatomyositis, acute rhabdomyolysis, and malignant hyperthermia. In many of the congenital structural myopathies, such as central core disease, nemaline rod myopathy, and fiber-type disproportion syndrome, a serum CK is likely to be normal or only mildly elevated.CK levels have ranged from normal to elevated two to four times in SMA I and II. SMA III patients have also been found to have normal to slightly elevated CK values, with elevations generally to two to five times normal.
A serum CK level greater than 10 times the upper limit of normal generally is exclusionary criteria for SMA and, in this setting, workup for other disorders such as inflammatory or dystrophic myopathies should be pursued. In a child with muscle weakness, a normal CK does not exclude a myopathy or other NMD conditions; however, a severely elevated CK is suggestive of but not diagnostic of a dystrophic myopathy or inflammatory myopathy.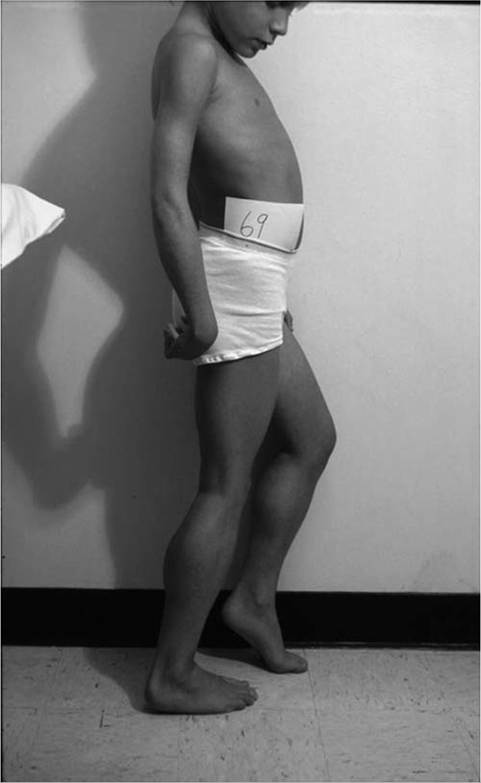
Figure 12.6 “Myopathic” stance in an eight-year-old male with Duchenne muscular dystrophy. Notice the lumbar lordosis to compensate for hip extensor weakness and primarily forefoot contact to compensate for knee extensor weakness.

Figure 12.7 Toe walking with initial floor contact in the transitional phase of ambulation in Duchenne muscular dystrophy is, in part, a compensatory mechanism to maintain knee stability.
Lactate and pyruvate levels are useful in the evaluation of possible metabolic myopathy. The presence of a lactic acidosis may be seen in such mitochondrial encephalomyopathies as Kearns-Sayre syndrome, myoclonic epilepsy and ragged-red fibers (MERRF) and mitochondrial encephalomyopathy with lactic acidosis and strokelike episodes (MELAS). Whenever clinical evidence suggests a disorder of oxidative metabolism, blood lactate and pyruvate levels should be obtained. Arterial lactate values are a more reliable guide. Stable or reduced levels of lactate and pyruvate, with con- comitany increases in ammonia with ischemic or nonischemic forearm exercise testing, suggests a mitochondrial dysfunction. In a setting of lactic acidemia, the lactate/pyruvate ratio may aid in the differential diagnosis. Children with suspected mitochondrial encephalomyopathy should be evaluated with cerebrospinal fluid (CSF) lactate and pyruvate levels, because these values are less subject to flux than are either venous or arterial values. The ischemic forearm test, initially utilized by McArdle, and the nonischemic forearm exercise test are widely used means of assessing muscle and aerobic metabolism in older, more cooperative patients (1,2).