Antibody ELISAs
Multiple antibody ELISAs have been evaluated, and Se and Sp estimates vary greatly within and between tests (Nielsen and Toft, 2008). It is therefore not possible to provide point estimates characterizing these tests.
They should preferably be evaluated prior to their specific use in a particular population.20.6.1 Detection of MAP-infected animals
Overall, the Se of antibody ELISA for detecting MAP-infected animals is low (~5-30%), but it increases with increasing age (Nielsen and Toft, 2006). Sp estimates are generally above 95% for commercial ELISAs.
20.6.2 Detection of MAP-infectious animals
The ability of antibody ELISAs to detect MAP- infectious animals depends on the test frequency (Fig. 20.1), the manufacturer and the cut- off chosen to deem the ordinal ELISA response ‘positive’ or ‘negative’. For example, when assuming that only animals with high-level continuous shedding can infect a susceptible animal, one can test such animals on different schedules to reduce the risk of transmission. As shown in Fig. 20.1, using the Pourquier milk ELISA (IDEXX, Montpellier, France) to test such animals daily, one can expect to detect 91% of infectious animals (time = 0 in Fig. 20.1). However, if the test is performed once per year, and this test date is 1 year prior to the start of the high-level continuous shedding, the Se would be 20% (Fig. 20.1, time = -1 year). In a third scenario, if such infectious animals were tested four times per year, 7091% would be detected (Fig. 20.1, time interval -0.25 to 0 years). This example illustrates the major impact of test frequency on the Se. The cumulative Se from repeated testing would be higher if at least one positive test result from the repeated test dates were considered sufficient to deem the animal positive.
Sp for the target condition ‘infectious’ can be interpreted as the probability that an animal will test negative given that it is not shedding MAP in doses deemed likely to cause infection in a susceptible animal.
It should be noted that a ‘non-infectious’ animal can be infected with MAP. Therefore, animals with MAP-specific antibodies with negative results from a sensitive microbiological assay can be considered MAP infected but not MAP-infectious.Some decision makers would prefer to confirm whether test-positive animals are MAP-infected or MAP-infectious, but it is not possible to exclude infection from an ELISApositive animal by use of ante-mortem tests. For example, for cows testing positive using the Pourquier milk antibody ELISA, only 50-60% would have culture-positive faecal samples within a year following a positive antibody test (Fig. 20.2, time interval 0-1 year). Some of the cows were therefore not MAP-infectious at the time that the antibodies were detected. However, the majority of cows would shed detectable amounts of MAP within 3.5 years of testing positive using the ELISA (Fig. 20.2, time interval 0 to 3.5 years). Therefore, cows that were antibody-positive but negative in culture would be considered MAP-infected but non-infectious. In practice, a microbiological test for infectious animals should only be used to determine whether an animal is shedding MAP at the time of testing. As illustrated by this example, a microbiological test for infectious animals should not be used to rule out MAP infection in an antibody-positive animal.
20.6.3 Detection of MAP-affected animals
ELISAs tend to perform well in confirming the presence of MAP infection in animals with a high pre-test suspicion of disease (e.g. persistent diarrhoea). For example, Weber et al. (2009) reported that the Pourquier serum ELISA had a Se of 0.830.92, at a Sp of 0.998. However, not all cows affected by MAP infection will experience diarrhoea, but they may experience reduced productivity. A combination of milk production data and antibody results can therefore be used to increase the diagnostic accuracy (Wang et al., 2006). Cows with fluctuating antibodies (i.e. fluctuating between test-positive and test-negative) may have increased milk production, whereas those with last-positive or repeated-positive test results may experience decreased milk production (Nielsen et al., 2009).
This decline may start 300 days prior to the occurrence of antibodies in some cows. To determine the MAP status of an animal, it may be necessary to evaluate both production data and ELISA results.20.6.4 Use of ELISA results on an ordinal scale
Results from antibody ELISAs are measured on an ordinal scale but are often dichotomized
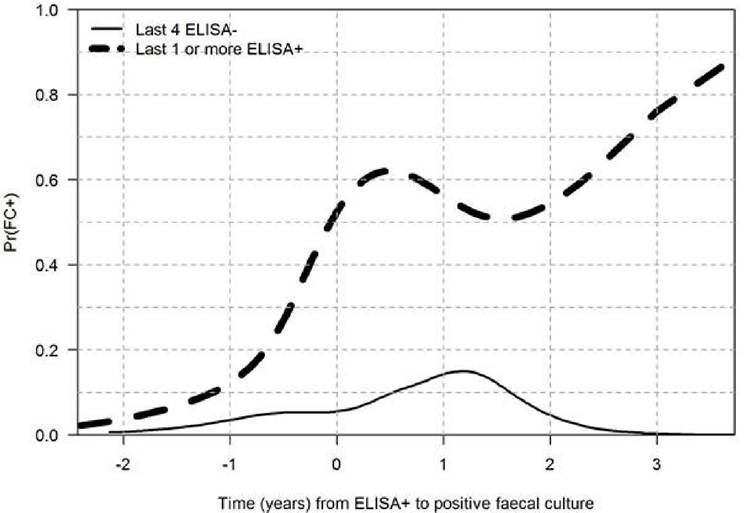
Fig. 20.2. Probability of testing positive in a faecal culture test relative to the time of testing positive in the commercial Pourquier milk enzyme-linked immunosorbent assay (ELISA) (using a cut-off sample-to- positive ratio of 30%).
to antibody-positive or antibody-negative results, making communication from the laboratory more straightforward. However, this simplification comes at the cost of a decrease in information, i.e. whether the ELISA values correlate with the probability of infection. Toft et al. (2005) estimated that cows with an optical density (OD) value of 0.3 had a 4% probability of shedding MAP, whereas if the cows had an OD value of 1.0, the probability of MAP shedding was 80% (Fig. 20.3). Therefore, there may be considerable advantages in using values on the ordinal scale, whether it is OD values or sample-to-positive ratios (S/P values) (Collins, 2002).
20.6.5 Predictive values of antibody ELISA
Single-antibody ELISA results may be of limited value (with the exception of prevalence estimates and herd certification) because animals with various antibody profiles are in different stages of MAP infection. Instead, results from frequent testing can better reveal the stage of infection as trends in results can be tracked over time. However, there is limited information on test evaluation in the context of repeated testing. Diagnostic test evaluations based on repeated tests are few, but two independent studies produced very similar age-specific test-sensitivity estimates (Nielsen et al., 2013; Meyer et al., 2018), with increases in the relative sensitivity from 0.3 at 2 years of age to 0.7 at 6 years of age in dairy cattle.
However, the repeated test results should rather be used based on their profile, e.g. two, three or more repeated positive tests would with increasing likelihood increase the probability that the cow is infected (Meyer et al., 2018). Current information suggests that the predictive properties of antibody ELISA are as shown in Table 20.3.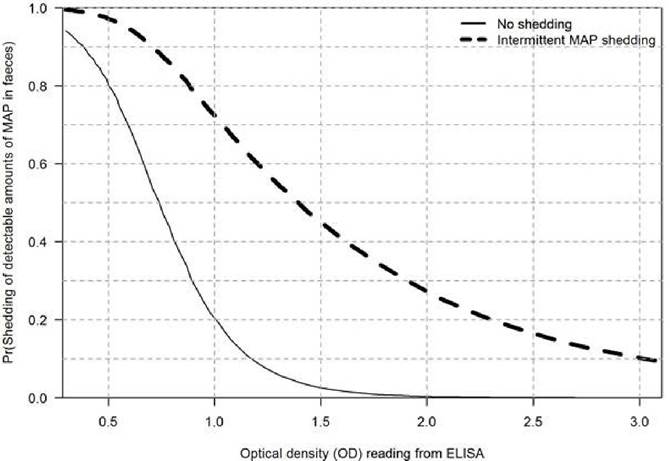
Fig. 20.3. Probability of detectable shedding of Mycobacterium avium subsp. paratuberculosis (MAP) in faeces. Values below the solid line show the probability of no MAP shedding at a given optical density (OD) value. Values between the solid and dashed line are probabilities of ‘intermittent’ MAP shedding, and values above the dashed line are probabilities of continuous MAP shedding. (Modified from Toft et al., 2005.)
Table 20.3. Prognostic properties of the antibody enzyme-linked immunosorbent assay (ELISA) for predicting Mycobacterium avium subsp. paratuberculosis (MAP)-affected, MAP-infectious, MAP- infected and non-infected adult cows.
| ELISA results | Predicted condition | |||
| Non-infected | MAP-infected | MAP-infectious | MAP-affected | |
| Repeated negative | Dependent on test history of herd | Possible in infected population | Rare | Rare |
| Fluctuating but last sample negative | Rare | Likely | Possible but likely to be low | Rare; a potential future event |
| Last sample positive | Rare | Very likely | Likely | Likely |
| Repeated positive | Rare | Very likely | Very likely | Likely; may be in near future |
20.7
More on the topic Antibody ELISAs:
- Being HIV antibody positive
- Twenty years after the first antibody test for the human immunodeficiency virus (HIV), highly active antiretroviral therapy (HAART) became available in Western countries.
- ANCA-Associated Vasculitis
- When is HIV counselling necessary?
- Pulmonary-Renal Syndromes
- Immunodeficiency
- The Tests
- Immunodiagnosis
- Blood transfusion and blood products
- Lymphogranuloma Venereum
- Appendix A Immunizations and Postexposure Therapies
- Since the global eradication of smallpox from May 8th, 1980, immunization has been established as the most cost-effective preventive measure against infectious diseases.
- Intestinal Plasmacytosis