Assessing the Eardrum
In many cases of chronic canine otitis media, the eardrum is ruptured as a result of long-standing otitis externa. Examination of the ears of a patient with chronic otitis media often reveals the absence of the eardrum.
The tympanic bulla may be filled with a dark material composed of epithelial cells, keratin, and cerumen (Figure 2-16). In acute suppurative otitis media, copious exudates resembling curdled milk are seen along the floor of the horizontal canal. Flecks of material are often seen floating in the liquid. After exudates and flush solution are suctioned from the external ear canal, the eardrum may not be visualized, but the bony tympanic bulla can be visualized beyond the annulus of the tympanic membrane. Many cases of otitis media are suspected due to the presence of an opaque eardrum or a bulging eardrum.It is difficult to assess the integrity of the eardrum if this structure cannot be clearly seen. When stenosis or occlusion of the ear canal prevents visualization of the eardrum, a rigid tomcat catheter can be advanced through the stenosis carefully. As the catheter is slowly advanced, it encounters a spongy object, the eardrum. If the eardrum is not ruptured and pressure is applied to the catheter, there is resistance.
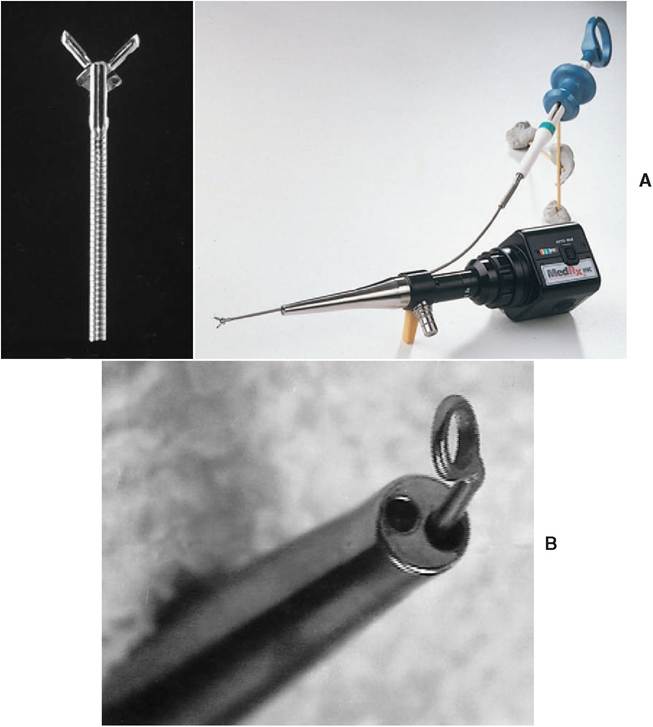
Figure 2-14
Using the working channel to work in the ear canal. A, An oval fenestrated endoscopic grasping forceps can be threaded through the Video Vetscope to remove foreign bodies, wax, polyps, and other material in the ear canal. B, Buck ear curette threaded retrograde into the 2-mm working channel of the Vetscope probe.
If the catheter advances, it will perforate the eardrum. If the catheter hits a hard object and does not advance, the object usually is the bone of the medial wall of the tympanic bulla, and the eardrum is not intact.
Sometimes when the eardrum is ruptured, using dilute povidone-iodine solution or fluorescein dye in the flushing solution will allow the colored solution to flush through the middle ear and out of the auditory tube. When this happens, the solution will come out of the nose or out of the back of the throat; the color indicates that there is a ruptured eardrum.

Figure 2-15
The Video Vetscope is assembled as a self-contained ear treatment station. (Courtesy MedRx,
Inc., Largo, Florida.)

Figure 2-16
Appearance of otitis media. Otoscopic examination of this Toy Poodle revealed the absence of most of the eardrum. The pars flaccida can be seen in the dorsal portion of the annulus. The tympanic bulla is filled with a dark waxy material composed of squamous epithelium, keratin, and cerumen.
Alternatively, if there is a small hole in the eardrum, the ear canal can be filled with normal saline with the patient in lateral recumbency and the affected ear facing upward. The video otoscope is advanced through the saline toward the eardrum. Any rising air bubbles indicate that air from within the tympanic cavity is escaping through a hole in the tympanic membrane.
Pathological changes may be present in the bulla and eardrum as indicated by opacity or discoloration of the intact eardrum (Figure 2-17). These findings signify either an ascending otitis media, which is common in cats but rare in the dog, or an otitis media in which the eardrum has healed over, leaving material within the tympanic bulla. There may be tissue in the bulla indicating a tumor mass or polyp. The eardrum may be reddened in response to inflammation or from accumulation of blood in the bulla. Whitish opacity indicates pus or mucus in the bulla, and yellow fluid indicates a serous effusion. A bulging membrane signifies fluid pressure behind the eardrum. Retraction of the eardrum around the malleus indicates negative air pressure. To relieve pressure gradients and obtain specimens from the middle ear for cytological evaluation and culture, a myringotomy should be done (Figure 2-18). (See Chapter 14, Otitis Media.)