Benign versus malignant lesions
When adequate numbers of tissue cells are present in a cytologic sample, morphologic characteristics are used to determine if the lesion could be benign or malignant. Characteristics of malignancy include anisocytosis, anisokaryosis, karyomegaly, binucleation, multinucleation, prominent or large nucleoli, multiple nucleoli, angular or elongated nucleoli, nuclear molding, abnormal nuclear shape, aberrant mitotic figures, atypical cytoplasmic vacuolation, increased nuclear to cytoplasmic (N:C) ratio, and dysmaturation of nuclear and cytoplasmic morphology (Figure 4.11).
The characteristics of malignancy involving the nucleus are considered more reliable than the cytoplasmic characteristics. In most cancers, a diagnosis of malignancy can be made if there are three or more cytologic characteristics of malignancy present (Raskin, 2023; Meinkoth et al., 2020). 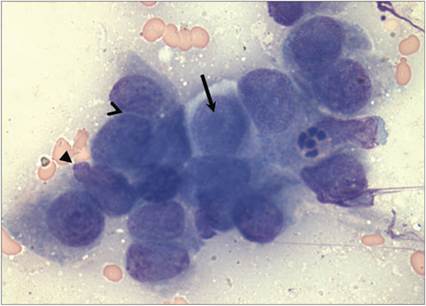
Figure 4.11 Malignant cells from a canine mammary carcinoma. Cells are large with scant to abundant basophilic cytoplasm, a large round nucleus, and stippled chromatin. A large nucleolus can be seen in some of the cells (arrow). Characteristics of malignancy include anisocytosis, anisokaryosis, cytomegaly, increased nuclear to cytoplasmic ratio, nuclear molding (open arrowhead), binucleation, and nuclear blebbing (closed arrowhead) (Wright–Giemsa, 1,000? magnification).
It is important to note, however, that some lesions can appear cytologically benign but have a very aggressive biologic behavior. For example, some well-differentiated malignant neoplasms, such as perianal gland tumors and thyroid tumors, may lack sufficient cytologic criteria of malignancy and may be difficult to distinguish from hyperplasia or their benign counterparts. It is also critical to recognize that cells in some lesions have criteria of malignancy but are simply dysplastic. In cases that contain both inflammatory and noninflammatory (tissue) cell types, dysplastic changes can occur in tissue cells that mimic characteristics of malignancy. This finding is common in lesions that are ulcerated or necrotic. It can be extremely challenging to distinguish dysplastic changes from the anaplastic changes caused by neoplastic cell transformation. This is why the presence of inflammation often precludes a definitive diagnosis of cancer on cytology. In these cases, biopsy with histopathology or repeat aspiration is necessary if the mass persists after resolution of the inflammation or the clinical suspicion of neoplasia is high. Mammary masses, in particular, are an important example of lesions that may be difficult to diagnose on cytology (see ‘Tumors of Glandular Structures – Mammary Masses’ section).