Cytologic appearance of lesions in skin and subcutaneous tissues
The cytologic appearance of aspirates from lesions in or under the skin can be grouped into very broad categories: acellular samples, samples containing cellular debris, bloody samples, inflammatory samples, or tissue samples (which may be normal, hyperplastic, or neoplastic).
If the sample is pauci- or acellular, the diagnosis of a cyst should be considered (Figure 4.7). More commonly, an acellular sample indicates that the aspirate was inadequate and repeat aspiration (potentially with suction applied) or biopsy with histopathology would be recommended. Cellular debris may be present because cells have been damaged during collection or because the lesion is necrotic. These samples are often non-diagnostic because cellular morphology cannot be adequately assessed. Aspiration of different areas of the lesion may be beneficial in these cases. 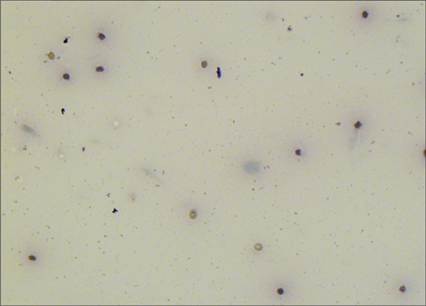
Figure 4.7 Cystic fluid in a skin mass from a 10-year-old domestic shorthair cat. There is a thin layer of proteinaceous material in the background of the slide. No nucleated cells are present. A few erythrocytes are seen (Wright–Giemsa, 500? magnification).
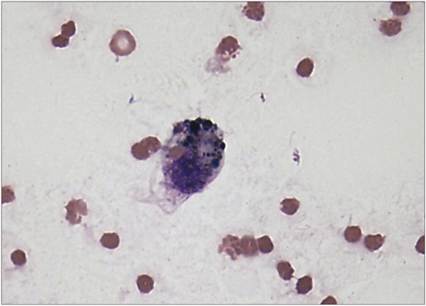
Figure 4.8 Hemosiderin-laden macrophage in an FNA of a hemorrhagic subcutaneous mass from a dog. The macrophage contains one visible erythrocyte and several variably sized, rounded, black pigment structures consistent with hemosiderin (Wright–Giemsa, 1,000? magnification).
If the sample contains intact cells, the cells need to be identified as peripheral blood cells, inflammatory cells, or cells representative of tissue/elements associated with the lesion. When there are large numbers of erythrocytes with low numbers of leukocytes and rare tissue cells, identification of the underlying pathologic process can be challenging.
Hemorrhage can be diagnosed in properly processed samples that contain a large amount of blood if erythrophagocytic and/or hemosiderin-laden macrophages are seen (Figure 4.8). Platelets are not observed in lesions with acute or chronic hemorrhage but may be seen during peracute hemorrhage. In samples that lack these features and contain platelets, it may be helpful to analyze a peripheral blood smear and a bloody cytology sample concurrently to determine if inflammation is present or if the sample is mostly peripheral blood. If the leukocyte density in the tissue aspirate is higher than the peripheral blood nucleated cell count, inflammation should be suspected. The inflammatory processes discussed in Chapter 2 (‘General Principles of Inflammation’) apply to lesions of the skin and subcutaneous tissues. Common causes of inflammation in these lesions are expanded on later in this chapter. If noninflammatory cells are present, the tissue type that the cells originated from is determined on the basis of cellular morphology. Most noninflammatory (tissue) cell types can be classified as epithelial, mesenchymal, or round cells.Epithelial cells typically are round or polygonal with distinct cell borders and round nuclei. They often are arranged in sheets or clusters with visible cell junctions (Figure 4.9). Cell junctions appear as distinct pale lines around the edges of adjacent cells. Mesenchymal cells are spindle-shaped or have wispy, indistinct cell borders with ovoid nuclei and usually are observed individually on the slide but may be aggregated together (Figure 4.10). Aggregates of mesenchymal cells lack cell–cell junctions and can appear intertwined, rather than being arranged next to each other, occasionally admixed with pink fibrillar extracellular matrix material. Mesenchymal cell aggregates can be difficult to distinguish from sheets of epithelial cells, which may prevent cytologic differentiation between tumor types. In these cases, clinical presentation, special stains, and biopsy with histopathology can help to determine the diagnosis (Andreasen et al., 1988; Hoinghaus et al., 2008).
Finally, round cells are individualized cells with rounded cytoplasm and round nuclei. The major round cell tumors and their distinctive cytologic appearances are described later in this chapter. 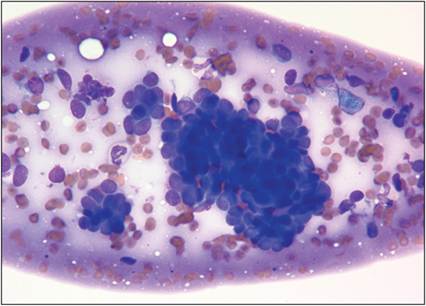
Figure 4.9 Epithelial cells are often clustered together. Cell–cell junctions can be seen as a thin, clear line between neighboring cells (Wright–Giemsa, 500? magnification).
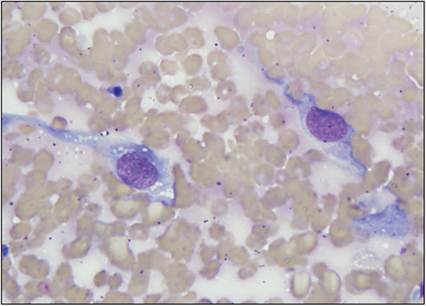
Figure 4.10 Mesenchymal cells in an FNA of a subcutaneous mass on the prepuce of a dog. Cells are large with abundant, spindle-shaped, basophilic cytoplasm and an oval nucleus with coarsely stippled chromatin. Small, distinct, clear cytoplasmic vacuoles and a prominent nucleolus are visible in the cell to the left. This patient was diagnosed with hemangiosarcoma (Wright–Giemsa, 1,000? magnification).