Poorly cellular, but diagnostic, samples
Cysts
Cystic structures usually palpate as firm, round masses in the dermis or subcutis. They form when cellular secretions or debris become entrapped under the skin. Collection of a clear to creamy fluid is expected during aspiration of a cyst.
Microscopically, the fluid appears as a thin basophilic or eosinophilic background in a cytologic sample (see Figure 4.7). Complete surgical removal of a cyst can be curative in dogs and cats.Epidermal inclusion cysts (epidermoid, follicular, or infundibular cysts)
Epidermal inclusion cysts form when keratinized epithelial cells fail to exfoliate and become trapped under the superficial epidermis. Aspirates of follicular cysts tend to have a thick, chalky appearance. Keratin debris (often seen as clumps of amorphous sky-blue material) and large numbers of anucleate, keratinized, squamous epithelial cells are present in these samples (Figures 4.12a, b). Also, clear rectangular cholesterol crystals (formed from the breakdown of cell membranes) are often identified (Figure 4.13). If nucleated squamous epithelial and/or basal epithelial cells are also present, then a follicular tumor is a possibility, as these tumors can have cytological characteristics similar to epidermal inclusion cysts (see the ‘Epidermal and Follicular Tumors’ section later in this chapter).
Figures 4.12 (a) FNA from a skin mass on the thorax of an 8-year-old dog. The sample is consistent with an epidermal inclusion cyst with a small amount of blood contamination. There are several polygonal blue anucleate keratinized epithelial cells. (b) Occasional cholesterol crystals (large rectangular nonstaining structures) also are observed (Wright–Giemsa: a, 200? magnification; b, 500? magnification).
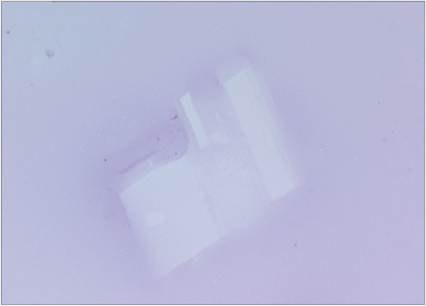
Figure 4.13 Cholesterol crystals can be found in epidermal inclusion cysts and lesions where cell degradation is occurring (Wright–Giemsa, 500? magnification).
When these cysts rupture and/or become inflamed or infected, neutrophilic to pyogranulomatous inflammation will be mixed in with the keratinized debris (Figure 4.14).
alt=fig4.14.jpg>
Figure 4.14 Inflamed epidermal inclusion cyst with numerous variably degenerate neutrophils, vacuolated macrophages, and pale blue keratinized debris (Wright–Giemsa, 500? magnification).
Sebaceous duct cysts
Sebaceous cysts form when proteinaceous product (keratin and sebum) is secreted into the center of a group of epithelial cells that line the mass. Grayish-white to brownish to yellowish cheese-like material can be released if the cyst becomes ruptured. Small clusters of benign-appearing epithelial cells that line the cyst may be present in the cytologic sample. If these cells are present, differential diagnoses include many of the, mostly benign, epithelial and adnexal tumors described later in this chapter.
Apocrine cysts
Occlusion of the sweat gland duct can lead to cyst formation. These can present as flocculant swellings and, when aspirated, can contain clear to brown-tinged fluid. Cytologically they are often acellular but can contain low numbers of cuboidal to columnar epithelial cells (Raskin & Conrado, 2023). These may be difficult to discern from cystic portions of an apocrine neoplasm.
Mammary cyst (mammary duct ectasia)
Mammary cysts may form as a result of dilated, distended ducts (Goldschmidt et al., 2011). They can be a dysplastic, non-neoplastic condition (most common in middle-aged to older female dogs), or may also be associated with neoplastic lesions. These cystic lesions aspirate as fluid, which may be brownish, yellowish, or red in appearance. Slides prepared from the cystic fluid typically contain proteinaceous background material and may also contain mammary secretory material, blood cells, macrophages, and/or foam cells. Cholesterol crystals (large, transparent, flat, rectangular crystalline structures often with a notch in one or more corners) are a common finding in many cystic lesions, including mammary cysts (Figure 4.15).
Clumps of epithelial cells may also be found in mammary cystic lesions. Benign and malignant mammary gland neoplasms may contain cystic areas (Figures 4.15, 4.16a–c), so if the lesion contains both solid areas and cystic areas, it is important to aspirate the solid portion to assess these more cellular areas for a potential neoplastic lesion. 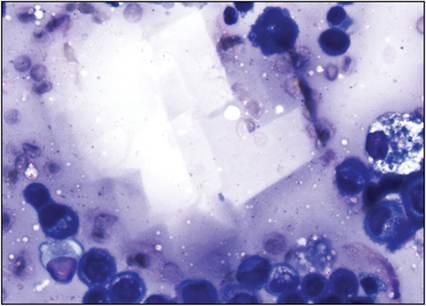
Figure 4.15 Cholesterol crystals from a cystic area in a mammary carcinoma in a 12-year-old, spayed female Doberman Pinscher (same lesion as Figures 4.16a–c). Cholesterol crystals typically appear as clear, flat, rectangular structures, often with a notch in one or more corners of the rectangle. They often appear in mica-like stacks (Wright–Giemsa, scale bar = 10 μm).
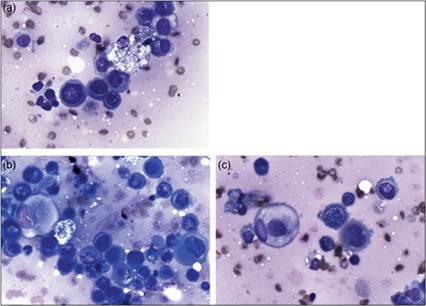
Figures 4.16a–c Epithelial cells (and foam cells) from a mammary carcinoma in a 12-year-old, spayed female Doberman Pinscher. Note that the epithelial cells have several criteria of malignancy, including a mitotic figure (a), anisocytosis and anisokaryosis, binucleation (c), and prominent nucleoli. They also appear more rounded which may reflect dissociation or exfoliation into fluid or anaplasia. The cholesterol crystals in Figure 4.15 are from a cystic area within this lesion (Wright–Giemsa, scale bar = 10 μm).
Tissue injury
Poorly cellular cytologic samples from damaged tissue may reflect aspiration of a hematoma, hygroma, or seroma. These samples may need to be centrifuged to adequately concentrate and evaluate any cells present. Hematomas are bloody fluids with low numbers of macrophages that contain phagocytized erythrocytes, blue-black pigment consistent with hemosiderin (a breakdown product of erythrocytes; Figure 4.8), and/or hematoidin crystals (diamond-shaped/rhomboid golden crystals, also an erythrocyte breakdown product).
A seroma is an accumulation of serous fluid within the skin, usually near a surgical incision site or area of previous trauma, and may contain low numbers of erythrocytes, occasional reactive macrophages with intracytoplasmic vacuoles, and rare to low numbers of neutrophils. No platelets are observed in hematomas or seromas, unless there is peracute hemorrhage or concurrent peripheral blood contamination. Hygromas are fluid-filled swellings that form over bony prominences (commonly the elbow) and pressure points, particularly in large-breed dogs. These lesions typically contain low numbers of macrophages and sometimes reactive fibrocytes (spindle-shaped mesenchymal cells).Sialoceles may appear as soft, fluctuant swellings, most commonly in the cranial cervical area or mouth, and form due to leakage of saliva into surrounding tissues of the face due to trauma or obstruction of the salivary duct. Please see Chapter 6 (‘Oral Cavity Cytology’) for further information on salivary gland and associated lesions.
Fibroplasia and desmoplasia
Proliferative, reactive fibroblasts can be seen as a reparative response to trauma/wounds in addition to irritation from local inflammation, foreign body, or neoplasia (i.e., scirrhous reaction). Cytology of reactive fibroblasts typically yields low numbers of individualized spindle cells sometimes associated with pink fibrillar matrix material. Spindle cells have scant to moderate amounts of basophilic cytoplasm and an ovoid nucleus with an open chromatin pattern and often small nucleoli (Figure 4.17). Moderate anisocytosis and anisokaryosis can be present as well as occasional binucleation, making it challenging to distinguish from mesenchymal neoplasia. Low numbers of spindle cells in the sample, numerous inflammatory cells, and the presence of individually occurring spindle cells with a low degree of atypia were recently identified as cytologic features encountered in fibroplasia compared to mesenchymal neoplasia (Masserdotti & Drigo, 2022).
Ultimately, correlation with clinical history and often histopathology are needed. 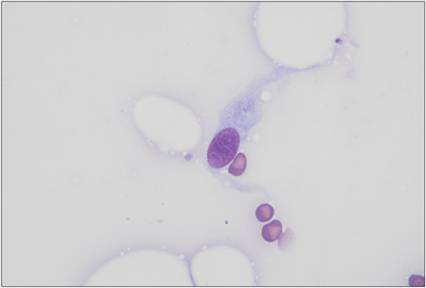
Figure 4.17 Reactive fibroblast in an FNA of a firm subcutaneous nodule at a previous surgical excision site from a dog. The cell is slightly plump with an ovoid nucleus with lacy chromatin and faint punctate nucleoli, and low amounts of thin, lightly basophilic, spindle-shaped cytoplasm (Wright–Giemsa, 1,000? magnification).
Calcinosis circumscripta and cutis
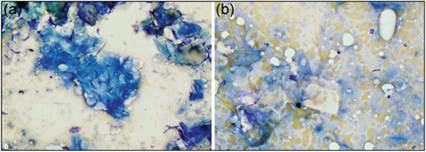
Minerals can be deposited in the skin secondary to trauma, mineral imbalances, and glucocorticoids (endogenous and exogenous). Calcinosis circumscripta can present as firm solitary lesions typically over joints, pressure points, bony prominences, or sites of previous trauma and are thought to be a result of dystrophic mineralization. Calcinosis cutis can present as gritty plaque-like lesions in the inguinal region as well as the dorsum and extremities, and it has been fairly well recognized in dogs with hyperadrenocorticism. Chalky white, gritty to pasty material may be discharged from these lesions. Smears of this material consist of a thick dense layer of lightly staining to nonstaining granular crystalline material with low numbers of cells such as macrophages and fibroblasts (Figure 4.18a, b). Inflammatory cells such as neutrophils, lymphocytes, and plasma cells may also be seen.
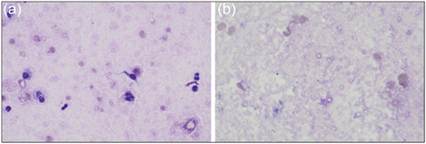
Figures 4.18a,b Calcinosis circumscripta. FNA of a 3–4 cm firm mass overlying the right scapula of a 9-month-old female intact Doberman Pinscher. There is abundant extracellular small rounded to irregular nonstaining crystalline material (mineral, a and b) with few erythrocytes and low numbers of vacuolated macrophages and rare mesenchymal cells (a) (Wright–Giemsa: a, 500? magnification; b, 1,000? magnification).