Inflammation and inflammatory lesions
Neutrophils
If neutrophils are the predominant cell type observed (>85%) in a cytologic sample and other inflammatory cells are less prevalent, the lesion is diagnosed as ‘neutrophilic inflammation’.
The terms ‘suppurative’ or ‘purulent’ have also been used to describe this type of inflammation. The morphologic appearance of the neutrophils may aid in diagnosis of the underlying cause of the inflammation (Figure 4.19). Degenerate neutrophils have karyolytic nuclei with pale, swollen chromatin and are suggestive of an underlying bacterial or fungal infection (Figure 4.20), such as can be seen with an abscess. If the neutrophils are nondegenerate (i.e., they appear similar to neutrophils found in peripheral blood samples), a sterile inflammatory process may be more likely (Figure 4.21). Causes of sterile inflammation include immune-mediated disease (e.g., pemphigus, cutaneous adverse drug reactions – discussed later in this chapter), caustic injury, and trauma. 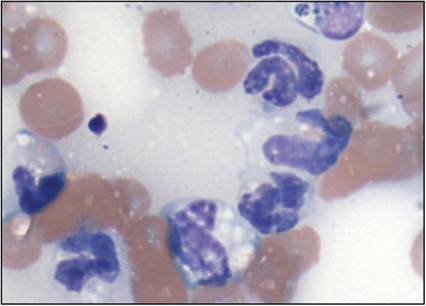
Figure 4.19 Degenerate neutrophils in a septic subcutaneous abscess from a dog. The nuclei of the segmented neutrophils are swollen and have a more open chromatin pattern than expected (Wright–Giemsa, 2,000? magnification).
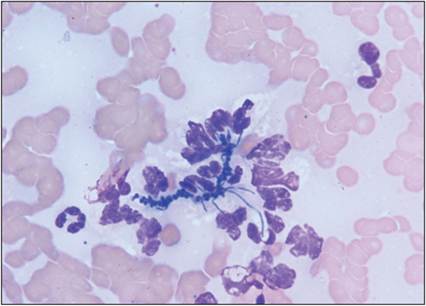
Figure 4.20 Degenerate neutrophils associated with Dermatophilus congolensis infection (Wright–Giemsa, 1,000? magnification).
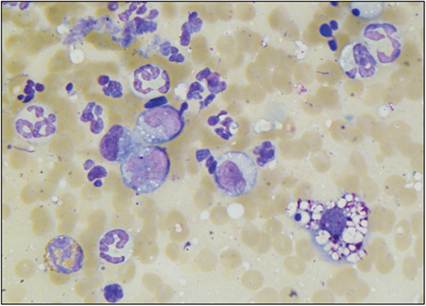
Figure 4.21 Mixed inflammatory reaction in a 1-cm mass on the left flank of a 9-month-old Bernese Mountain Dog. Several neutrophils and erythrocytes, lower numbers of macrophages, an eosinophil, and a lymphocyte are present.
Nondegenerate neutrophils have nuclei that are dense with crisp edges, similar to neutrophils in peripheral blood smears (Wright–Giemsa, 1,000? magnification).
Karyorrhectic and pyknotic neutrophils (which have clumped, fragmented, and condensed chromatin) suggest a chronic inflammatory process (Figures 4.22a, b). Chronic inflammation is also suspected when low numbers of macrophages are observed along with large numbers of neutrophils. When an infectious organism can be identified within the cytoplasm of neutrophils or macrophages (intracellular), the lesion can be classified as ‘septic’ (Figure 4.23), not to be confused with sepsis and septicemia (unless identified in the blood). If an organism cannot be identified, the cause of disease is less certain. Recent or ongoing administration of antimicrobials can prevent the cytologic diagnosis of bacterial infection. If clinically relevant, bacterial and/or fungal culture should be performed when inflammation is observed even if the neutrophils appear nondegenerate.
Figures 4.22a,b Chromatin condensation in cells in a septic subcutaneous abscess from a dog. (a) The nucleus of the cell in the center of the image with four areas of condensed chromatin is karyorrhectic. (b) A pyknotic cell with a single spot of condensed chromatin is shown at the center of the image. The cell contains several bacterial rods. Degenerate neutrophils are also present in both images (Wright–Giemsa, 2,000? magnification).
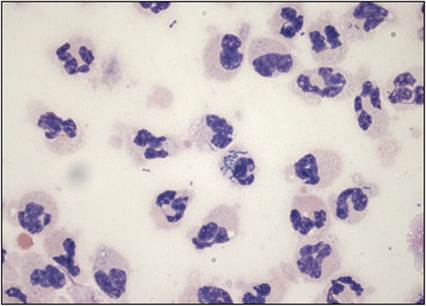
Figure 4.23 Septic suppurative inflammation. Several mildly degenerate neutrophils are present. One of the cells in the center contains several bacterial cocci and rare bacterial rods. A few extracellular bacteria can also be seen (Wright–Giemsa, 1,000? magnification).
Histiocytes
The term histiocyte is used generically to describe cells of the macrophage or dendritic (e.g.
Langerhans cells (LC) and interstitial dendritic cells) lineage (Moore P.F., 2023). These cells are characterized as large mononuclear cells with modest amounts of basophilic cytoplasm that may contain vacuoles and a paracentric to eccentric rounded to lobulated nucleus.Macrophages
When the majority of cells in a cytologic sample are macrophages, the lesion is diagnosed as ‘macrophagic’ or sometimes ‘histiocytic’ inflammation. On histopathology, the presence of these large mononuclear cells in conjunction with epithelioid macrophages (macrophages with a more rounded to polygonal appearance, resembling epithelial cells) with or without multinucleated giant cells is consistent with ‘granulomatous’ inflammation. Multinucleated giant cells in inflammatory lesions should not be interpreted as neoplastic cells (Figure 4.24). Causes of granuloma formation include foreign body reaction, fungal infection, atypical bacterial infection, and chronic inflammation. Classic examples of diseases that induce granulomatous inflammation include histoplasmosis (Figure 4.25) and mycobacterial infections (Figures 4.26a,b).
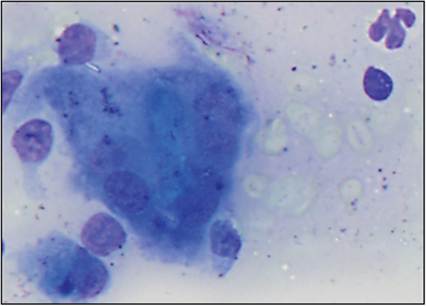
Figure 4.24 Multinucleated giant cell in an FNA from a subcutaneous granuloma in a dog. A large multinucleated macrophage is shown. Other cell types present include erythrocytes, macrophages, a degenerate neutrophil, and two lysed cells that lack cytoplasm (Wright–Giemsa, 2,000? magnification).
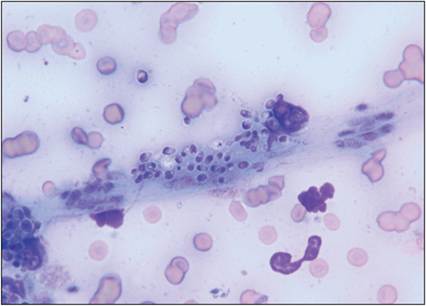
Figure 4.25 Histoplasma capsulatum organisms are small 1–2 μm diameter yeast structures with a thin distinct clear cell wall and often a crescent-shaped nucleus. The organisms in this image are associated with a ruptured cell but typically organisms are observed within macrophages (Wright–Giemsa, 1,000? magnification).
Figures 4.26a,b Mycobacterial infection.
(a) FNA of a subcutaneous mass from a cat. The image shows several macrophages that contain nonstaining bacterial rods. A few partially intact neutrophils and rare erythrocytes also are present. Extracellular bacterial rods can be observed against the basophilic proteinaceous background of the sample. (b) FNA of a nasal mass from a cat. The image shows several macrophages that contain nonstaining bacterial rods. Several intact neutrophils and low numbers of erythrocytes also are present (Wright–Giemsa, 1,000? magnification).
Reactive histiocytoses
In dogs and cats, the majority of histiocytic disorders involve proliferations of cells of LC or interstitial dendritic cell lineage. There are several subtypes of histiocytic disorders (Affolter & Moore, 2000; Affolter & Moore, 2002; Moore et al., 2006; Moore P.F., 2023). Currently, cutaneous histiocytosis (CH) and systemic histiocytosis (SH) are considered non-neoplastic, inflammatory diseases. CH and SH are referred to as the ‘reactive histiocytoses’ and have only been identified in dogs. Histiocytoma, canine cutaneous Langerhans cell histiocytosis (LCH), feline progressive histiocytosis, and histiocytic sarcoma are neoplastic diseases, discussed later in this chapter (see ‘Histiocytic Neoplasms’).
CH and SH are histiocyte and lymphocyte-rich inflammatory disorders associated with a degree of immune dysregulation and are due to abnormal accumulation of activated dermal interstitial dendritic cells (Moore, 2014; Moore P.F., 2023). Cells appear similar to macrophages and have abundant lightly basophilic cytoplasm and an ovoid nucleus with finely stippled chromatin. Neutrophils and small lymphocytes are also observed. If dermal dendritic cells form masses in the skin and subcutis, the disease is called ‘cutaneous histiocytosis’, and the local lymph nodes can also be affected. In systemic histiocytosis, the lesions are diffuse and are typically found in the skin, ocular and nasal mucosa, and sometimes the internal organs (Mays & Bergeron, 1986; Moore P.F., 2023).
Affected animals have multiple skin lesions that wax and wane. Long-term immunosuppressive treatment is often needed for these patients (Coomer & Liptak, 2008).
Neutrophils and macrophages
When a lesion contains a mixed population of neutrophils and macrophages, it may be described as ‘neutrophilic and macrophagic’ or ‘pyogranulomatous’ inflammation. The macrophages associated with granulomatous and pyogranulomatous inflammation are often described as epithelioid because of their similar appearance to epithelial cells. The list of differential causes for pyogranulomatous inflammation is similar to the list for granulomatous inflammation (foreign body reaction, fungal infection, atypical bacterial infection, and chronic inflammation).
Close examination of these samples for fungal elements and filamentous bacteria is warranted. Examples of infectious organisms associated with pyogranulomatous inflammation include Pythium insidiosum (Figure 7.32 in Chapter 7, ‘Cytology of the Gastrointestinal Tract’), Lagenidium spp., Blastomyces dermatitidis (Figure 4.27), Coccidioides immitis (Figure 12.16b in Chapter 12, ‘Musculoskeletal Cytology’), Histoplasma capsulatum (Figure 4.25), Sporothrix schenckii, and Nocardia spp. (Figure 4.28). Special stains such as silver and periodic acid–Schiff stains can be helpful to highlight organisms if they are not seen using a routine Romanowsky-type stain (Figure 4.29).
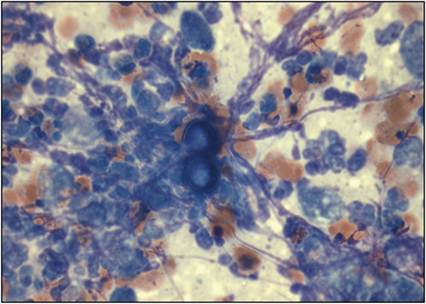
Figure 4.27 Pyogranulomatous inflammation due to blastomycosis. Imprint cytology of a draining skin lesion from a dog. The sample contains several degenerate neutrophils, lower numbers of macrophages, and large (17–22 μm), round, yeast structures. The organism has a deeply basophilic nucleus, a distinctive double-contoured capsule, and exhibits broad-based budding consistent with Blastomyces dermatitidis. There is also nuclear streaming present (linear purple strands), not to be confused with fungal hyphae (Wright–Giemsa, 1,000? magnification).
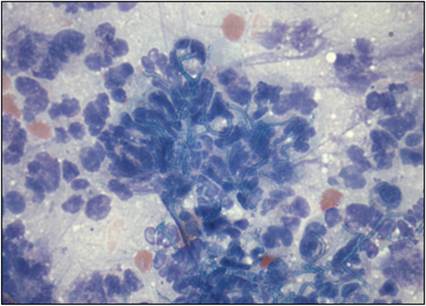
Figure 4.28 Pyogranulomatous inflammation due to nocardial infection. Multiple subcutaneous masses from an immunosuppressed dog were aspirated. Several branching, thin, filamentous organisms were entrapped within large numbers of degenerate neutrophils and fewer macrophages. Culture for anaerobic bacterial and fungal organisms yielded Nocardia abscessus (Wright–Giemsa, 1,000? magnification).
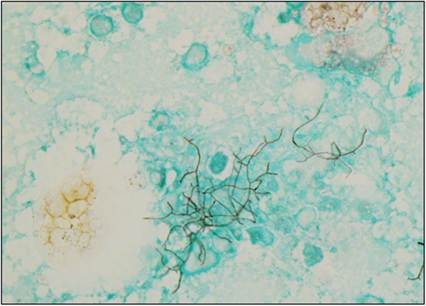
Figure 4.29 FNA of a subcutaneous mass from a 4-year-old Bichon Frise. The dark golden-brown branching structures are Nocardia spp. organisms. This stain would also highlight fungal elements (Grocott’s methenamine silver, 100? magnification).
Fungal organisms can be present as yeast (rounded to ovoid structures) and/or hyphae (linear structures, often with septations, occasionally branching), not to be confused with debris or nuclear streaming. Some organisms have distinct cytologic features. The yeast form of Blastomyces dermatitidis (Figure 4.27) ranges from 8 to 22 μm and has a double-contoured wall and broad-based budding. These organisms are deeply basophilic and easily identified in cytologic preparations. Coccidioides immitis organisms appear as variably sized, thick, basophilic spherules (20–200 μm) with a thick blue to purple wall and a granular internal structure (due to the presence of endospores). The endospores are round, 2–5 μm in diameter, and can be confused with Histoplasma spp. when seen extracellularly (Fisher, 2020; Raskin & Conrado, 2023). Histoplasma capsulatum (Figure 4.25) is a much smaller organism (approximately 2 μm) and is often phagocytized by macrophages. It is rounded, has a thin clear cell wall, and contains a crescent-shaped eosinophilic nuclear structure. Sporothrix schenckii can appear similar to Histoplasma spp.; however, some organisms have more of an elongate, fusiform shape. Pythium insidiosum and Lagenidium spp. are waterborne fungus-like organisms, and infection typically causes pyogranulomatous inflammation with an eosinophilic component in the gastrointestinal tract and less commonly in the skin (observed as cutaneous nodular ulcerated lesions). Cytology preparations show the presence of poorly staining, poorly septate, broad, branching hyphae (Fisher, 2020; Raskin & Conrado, 2023).
Neutrophilic and macrophagic inflammation can also be seen with reactive fat (panniculitis), where subcutaneous fat becomes inflamed secondary to trauma, foreign bodies, vaccines, infection, and idiopathic causes. Panniculitis presents as subcutaneous or deep cutaneous nodules. Aspirates consist of mature adipocytes, extracellular free lipid, lipid-laden rounded to spindled cells (macrophages and/or fibroblasts), and variable numbers of neutrophils. These cytological findings may be difficult to discern from an inflamed lipomatous mass.
Eosinophils
‘Eosinophilic inflammation’ is diagnosed in cytologic samples that contain >10% eosinophils (Figure 4.30). Eosinophils are not commonly seen in the blood or tissue; therefore, even low numbers of eosinophils are considered significant. Frequently, significant numbers of neutrophils and/or macrophages are also present in these lesions. This type of inflammation is associated with parasites, allergic diseases, type I hypersensitivity reactions (e.g., due to insect bites or stings), immune-mediated diseases, and paraneoplastic conditions. Eosinophilic inflammation is supportive of a diagnosis of eosinophilic granuloma, which is one of the most distinct and common manifestations of eosinophilic granuloma complex (EGC) in cats that have a raised, erythematous, alopecic mass. The other clinical presentations of ECG are eosinophilic plaques and indolent (rodent) ulcers. Some other differentials for eosinophilic plaque or granuloma are infectious agents (e.g., demodecosis, fungal and fungal-like infections) and a paraneoplastic response to certain tumors such as mast cell tumors, lymphomas, and carcinomas (Raskin & Conrado, 2023).
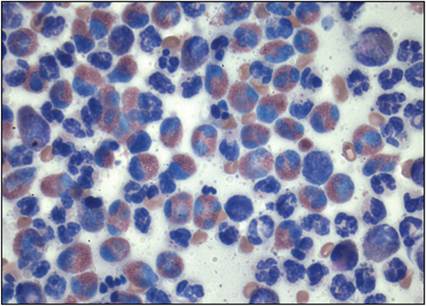
Figure 4.30 Eosinophilic inflammation in a hairless, raised, erythematous, dermal lesion from a cat. There are large numbers of eosinophils filled with eosinophilic cytoplasmic granules. Large numbers of neutrophils also are present (Wright–Giemsa, 1,000? magnification).
Lymphocytes
In lesions diagnosed as ‘lymphocytic inflammation’, the majority of cells are small, well-differentiated lymphocytes. Additionally, low numbers of intermediate-sized lymphocytes are expected to be present in these lesions. If plasma cells are also observed, the term ‘plasmacytic–lymphocytic’ or ‘lymphoplasmacytic’ inflammation is used (Figure 4.31). Antigenic stimulation is the most common cause of both lymphocytic and plasmacytic–lymphocytic inflammation. Examples of sources of antigen include insect bites, vaccines, and viral infections. Delayed (type IV) hypersensitivity reactions should be considered when lymphocytic or plasmacytic–lymphocytic inflammation is observed.
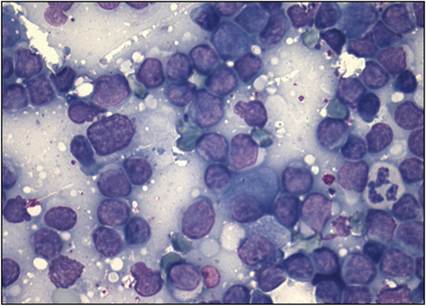
Figure 4.31 Plasmacytic–lymphocytic inflammation in an FNA of a small, firm, subcutaneous mass from a cat. The majority of cells are small lymphocytes with a nuclear diameter less than the diameter of the neutrophil. A few intermediate-sized lymphocytes with nuclei approximately the diameter of the neutrophil are present. One plasma cell also is shown at the center of the image (Wright–Giemsa, 1,000? magnification).
Mixed inflammation
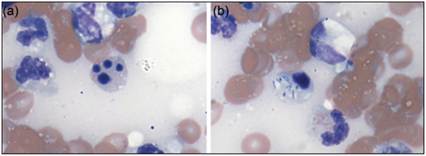
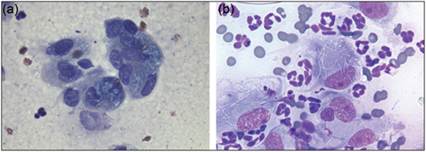
Cytologic samples may contain large numbers of neutrophils, macrophages, and lymphocytes (with or without rare eosinophils). These lesions are diagnosed as ‘mixed inflammation’ to indicate that many inflammatory cell types are present. Chronic inflammation, acral lick dermatitis/lick granulomas, and vaccine reactions are commonly associated with a mixed inflammatory response. In vaccine reactions, brightly eosinophilic to magenta globular material can often be seen within macrophages (Figures 4.32a, b). Blue or blue–gray globular material may also be seen within macrophages, and is associated with the use of vaccines that have a metal-containing adjuvant (e.g. certain rabies vaccines; Scruggs & LeBlanc, 2015).
With mastitis, cytological preparations of mammary secretions or aspirates contain predominantly neutrophils that may be degenerate, or variable numbers of neutrophils, lymphocytes, and macrophages depending on the causative agent. If due to an infection, organisms (most commonly bacteria) may be seen within neutrophils and macrophages (Fisher, 2020).
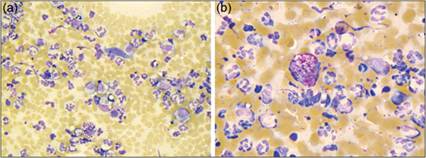
Figures 4.32a,b FNA of a 1 cm mass on the left flank of a 9-month-old Bernese Mountain Dog. Several neutrophils, lower numbers of macrophages, rare lymphocytes and fibroblasts, and several erythrocytes are present. Some macrophages contain bright eosinophilic globular material consistent with vaccine adjuvant (Wright–Giemsa: a, 500? magnification; b, 1,000? magnification).