Dermatologic cytology
This section provides a brief review of the common non-neoplastic dermatologic lesions, some of which are discussed in other parts in this chapter. These skin lesions can be infectious or noninfectious, inflammatory or noninflammatory, and can be evaluated via cytology using a variety of sample collection techniques such as needle aspirates, scrapes, swabs, and impression smears (see Chapter 1, ‘Sample Acquisition and Preparation’).
This review focuses on microbial overgrowth, dermatophytosis, mite infestation, and pemphigus foliaceus. Other noninfectious, inflammatory lesions, such as cutaneous adverse drug reactions, foreign body reactions, vaccine reactions, and acral lick dermatitis, are mentioned in the ‘Mixed Inflammation’ section. For additional dermatologic information, the readers are directed to the references.Low numbers of bacteria and few fungi can be found on the skin surface in health, as part of the normal microbiota. Bacterial or fungal overgrowth and secondary skin infections can be seen when there is compromise of the skin barrier (e.g., trauma, inflammation) or immunosuppression, and affected patients can present with pruritus, erythema, and scaling (Albanese, 2017). Cytology samples of microbial overgrowth will have significantly increased numbers of microbes and may or may not contain inflammation (Figure 4.33). When inflammation is present, it could represent pyoderma or an abscess. Superficial pyoderma commonly presents as cutaneous pustules, papules, erosions, moist exudation, crusts, and erythema, while deep pyodermas (e.g., bacterial folliculitis and furunculosis) can present as ulcers, swellings, nodules, and draining tracts. Staphylococcus spp. is most commonly involved. Other bacterial pathogens may also cause pyoderma, such as Streptococcus spp. and rods such as Escherichia coli, Pseudomonas species, or Klebsiella spp.
(Welle & Linder, 2021). Neutrophilic inflammation or a mixed inflammatory response (neutrophils and macrophages +/– lymphocytes) is typically observed on cytology with pyoderma, and neutrophils may appear degenerate and contain phagocytized bacteria. Deeper pyodermas can also contain fragments of keratin extracellularly as well as within macrophages and sometimes few acantholytic keratinocytes. Bacterial abscesses typically have many degenerate neutrophils and bacteria may be seen extracellularly and within neutrophils (Figures 4.19, 4.22a–b, 4.23). 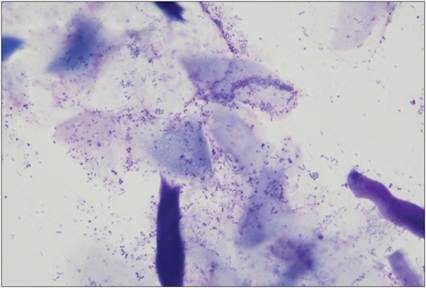
Figure 4.33 Bacterial overgrowth. Three-year-old English Bulldog with moderate cutaneous erythema and exudate of tail fold skin. Impression smear cytology revealed numerous anucleate squamous epithelial cells, keratin, keratinaceous debris, and bacteria (paired cocci and rods) without inflammation. This patient was previously diagnosed with atopic dermatitis of unknown etiology (Diff-Quik®, 1,000? magnification).
Cutaneous fungal overgrowth is more commonly attributed to Malassezia species than Candida. On cytology, Malassezia appears as small (3–8-μm) oval to peanut or foot-print shaped, broad-based budding organisms (Figures 18.2, 18.35 in Chapter 18, ‘Cytology of the Ear’), which are extracellular or may be adhered to the surfaces of keratinized squamous epithelial cells. Finding greater than two organisms per high power field (100? oil objective) is suggestive of Malassezia overgrowth (Fisher, 2020). A mixed inflammatory response (lymphocytes and macrophages) may be seen with Malassezia dermatitis, in addition to neutrophils if secondary pyoderma develops (Raskin & Conrado, 2023). Candida is a commensal that is found in the GI tract and mucous membranes but can cause mucocutaneous or cutaneous disease, particularly in immunosuppressed animals. This organism can appear as small (2–10-μm) ovoid yeast organisms that bud or have elongate germ tube formation with pseudohyphae and sometimes true hyphae (Figures 6.14 and 7.30a–c in Chapters 6, ‘Oral Cavity Cytology’, and 7, ‘Cytology of the Gastrointestinal Tract’).
Other important dermatologic etiologic agents, some of which are zoonotic, include ringworm or dermatophytosis and mite infestation. Dermatophytosis can be diagnosed via trichogram (hair pluck, prepared with mineral oil or 10–20% potassium hydroxide solution); some lesions may also fluoresce with a Wood’s lamp (UV light). On cytology, fungal arthrospores (small round to ovoid structures) may be visualized within hair shafts (endothrix, e.g., Trichophyton mentagrophytes; see Figure 4.69a) or on the hair shaft surface (ectothrix, e.g., Microsporum canis or M. gypsum); hyphae may also be seen. Mite infestation can be caused by Demodex (demodectic or follicular mange), Sarcoptes (canine scabies), Notoedres (feline scabies), and Cheyletiella. Low numbers of Demodex can be found in the skin but increases can result in clinical signs such as pruritus and alopecia. These organisms are found primarily within hair follicles, have an elongate cigar shape, eight legs (nymphs and adults; Figure 18.5 in Chapter 18, ‘Cytology of the Ear’), and are best visualized on deep skin scrapes performed in the middle of the lesions. Demodecosis can have a cytologic appearance similar to deep pyoderma, as secondary bacterial infections can develop. Canine scabies is caused by Sarcoptes scabei var. canis and adults are ovoid and measure 200–400 μm in diameter with four paired short legs (Figure 4.34; Miller et al., 2013). Lesions associated with infestation include papules, areas of erythema, crusting, and alopecia. Multiple superficial skin scrapes should be collected to increase the chance of detecting the mites in dogs with suspected scabies. Feline scabies is caused by Notoedres cati, which is similar in morphology but smaller than Sarcoptes (Miller et al., 2013). Unlike canine scabies, often many mites are visualized on skin scrapes from cats with scabies. Cheyletiellosis is termed ‘walking dandruff’ because mites can be grossly seen moving along the skin of infected animals.
They are highly contagious and can spread to other animals and humans. Animals may be asymptomatic or can have dry scaling (appears similar to dandruff) along the dorsum, alopecia, crusting, and pruritus. Tape impressions, examination of hair and scale samples, and flea combs are some methods used to identify mites, which have four pairs of legs with combs and characteristic accessory mouthparts that terminate in prominent hooks (Figure 4.35; Miller et al., 2013). Otodectes, an aural mite, is discussed in Chapter 18 (‘Cytology of the Ear’). Fleas can also incite an allergic dermatitis with gross lesions of papules, crusts, alopecia, and erythema (Albanese, 2017). Cytologically these lesions commonly contain mostly eosinophilic inflammation with variable numbers of mast cells, basophils, and macrophages. This cytologic pattern can also be seen with atopic dermatitis, food allergy, and other arthropod-bite/sting (e.g. mosquito). 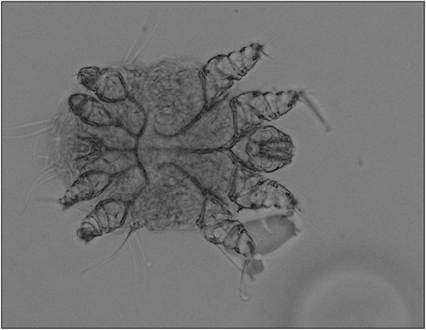
Figure 4.34 Sarcoptes spp. adult mite. (Unstained, 200? magnification; image courtesy of Dr. Roxanne Charles.)
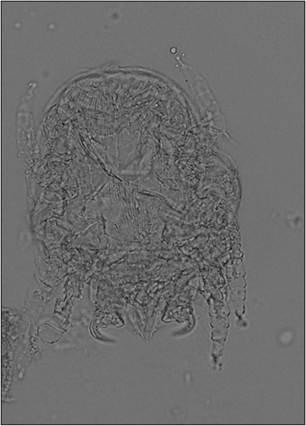
Figure 4.35 Cheyletiella spp. adult mite. (Unstained, 200? magnification; image courtesy of Dr. Roxanne Charles.)
Autoimmune skin disease is uncommon in dogs and cats and typically requires biopsy with histopathology for diagnosis. Two important autoimmune complexes include pemphigus and lupus. Pemphigus complex includes pustular and blistering disorders – pemphigus foliaceus, pemphigus vulgaris, pemphigus vegetans, and pemphigus erythematosus. Within this complex, pemphigus foliaceus is the most common, and typically presents as pustules that eventually progress to form crusts. Cytology of these lesions contains non-degenerate neutrophils and many acantholytic cells (individually occurring keratinocytes that are round/oval to polygonal in shape, have deeply basophilic cytoplasm, and a round centrally located nucleus) are observed (Figure 4.36).
Eosinophils may also be seen with this disease (Albanese, 2017). While acantholytic cells can be supportive of pemphigus, they can also be seen (albeit in lower numbers) with bacterial pyoderma and dermatophytosis, so thorough examination for infectious agents is recommended. The lupus complex includes discoid lupus erythematosus (DLE) and systemic lupus erythematosus, with DLE primarily affecting the skin. DLE lesions typically involve the face (around the nose and eyes) and footpads and may include erythema, depigmentation, ulceration, or erosion (Miller et al., 2013). Biopsy is considered the diagnostic method of choice, coupled with clinical signs and antinuclear antibody testing. Additional discussion on SLE can be found in Chapter 12 (‘Musculoskeletal Cytology’). 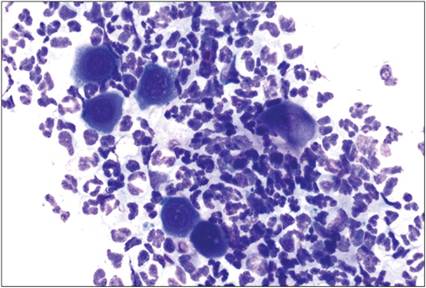
Figure 4.36 Pemphigus foliaceus. Impression smear of moist erythematous lesions under cutaneous crusts in a 13-year-old Miniature Schnauzer with diffuse dermatitis. There are numerous variably degenerate neutrophils and modest numbers of individualized squamous epithelial cells. Several epithelial cells appear acantholytic with a more rounded appearance and deeper blue cytoplasm (Diff-Quik®, 500? magnification).