Bladder
Sampling
Cytology of urinary bladder tissue is generally reserved for investigation of masses and suspected neoplastic disease. Most inflammatory lesions affecting the bladder can be diagnosed via urine sediment examination, a minimally to non-invasive procedure for the patient.
Ultrasound-guided FNAs can be used to sample thickened bladder walls and intraluminal masses. However, the most common neoplasm of the bladder is UC and neoplastic cells from UCs can seed needle tracks after FNA attempts (Nyland et al., 2002), as well as open surgical procedures (Higuchi et al., 2010). Many clinicians, therefore, prefer the traumatic catheterization technique to obtain cells from intraluminal bladder masses.
Traumatic catheterizations are performed under deep sedation or a short general anesthesia, with the patient in lateral or ventral recumbency. A urinary catheter is introduced into the bladder in a sterile fashion. The bladder is emptied and the mass (usually in the trigone) is located. Rectal palpation or ultrasound guidance may be needed to localize the catheter to the mass/trigone region. If the mass is further away than the trigone, it may not be accessible via this method. Apply negative pressure to the catheter with a 10 or 20 ml syringe. While holding the negative pressure, move the catheter back and forth, rubbing against the tumor. Small pieces of tumor and blood will be seen in the catheter and syringe. Direct and sediment smears of the retrieved fluid should be prepared, but the most cellular and diagnostic samples tend to come from squash preparations of small tumor pieces. If tumor pieces are large enough, they can be placed into formalin and submitted for histopathology instead. (Procedural information contributed by Cecilia S. Robat, DVM, DACVIM [Oncology].)
Imprints of biopsied tissue may also be used for cytologic evaluation.
If small samples are obtained via cystoscopy or traumatic catheterization, imprints will be difficult to make and could damage the tissue. The best option in these cases may be to leave the tissue untouched to ensure a more accurate histologic examination. Larger pieces of tissue obtained via cystotomy are better candidates for tissue imprints.Normal
Healthy urinary bladders are typically not sampled for cytology but normal/unremarkable urothelial cells (also known as transitional epithelial cells) may be retrieved when investigating pathologic conditions. Depending on the sampling method, specimens will be poorly to moderately cellular, with catheterized samples being more cellular than aspirates or free catch methods. Urothelial cells may be found individually and in small clusters (Figure 10.16). These cells are cuboidal with a moderate amount of lightly basophilic cytoplasm. Nuclei are round to oval and often contain patchy chromatin from being exposed to urine. Mild anisocytosis is considered a normal finding in urothelial epithelium. Anisokaryosis will be minimal. A small amount of blood with associated leukocytes may also be retrieved.

Figure 10.16 A cluster of unremarkable urothelial epithelial cells from a catheterized routine urinalysis (modified Wright’s, 600? magnification).
Inflammation
Most cases of cystitis are diagnosed based on history, physical examination findings, and urine sediment examination. However, neutrophilic inflammation and bacterial infection can accompany neoplastic disease in the bladder. In addition, chronic infection and inflammation can result in significant, even mass-like, urothelial hyperplasia. Therefore, bacterial organisms and neutrophilic inflammation may be identified when sampling various mass lesions (Figure 10.17). This combination of factors can make interpretation of cytology difficult and is discussed further in the later hyperplasia section.
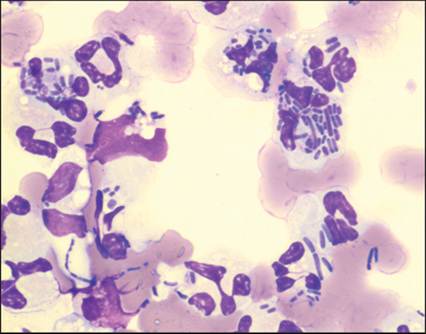
Figure 10.17 Septic neutrophilic (suppurative) inflammation in a dog. This patient presented for a mass lesion in the bladder and was eventually diagnosed with urothelial carcinoma. Initial sampling, however, only retrieved a secondary urinary tract infection (modified Wright’s, 1,000? magnification).
Neoplasia
Urothelial carcinoma (UC) is the most common neoplasm to affect the urinary bladder in both dogs and cats, although the incidence in cats is very low compared to dogs (Griffin et al., 2019). In both species, UC most commonly affects the trigone region. The gross appearance can vary in morphology from a papillary mass to a thickened bladder wall. UCs that arise in the bladder may extend into the urethra or prostate (Knapp & McMillan, 2010).
Samples from UCs, particularly squash preparations from traumatic catheterizations, can be moderately to highly cellular with urothelial cells in small clusters and large sheets (Figure 10.18). Although typically less cellular than catheterized samples, voided urine samples may have increased urothelial cellularity to suggest neoplastic disease. Some UCs contain epithelial cells similar to normal urothelial cells (i.e. cuboidal cells with a moderate amount of basophilic cytoplasm and round central nuclei [Figure 10.19]). These cells may have an increased N:C ratio and mild pleomorphism that raises the suspicion for neoplasia, but a definitive diagnosis may not be possible by cytology alone.
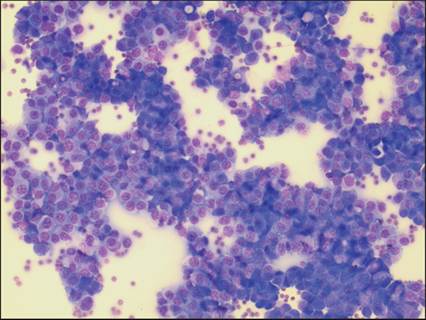
Figure 10.18 Urothelial carcinoma. Squash preparation from traumatic catheterization procedure. Low-power view demonstrating the high cellularity that can be retrieved via this sampling method (modified Wright’s, 200? magnification).
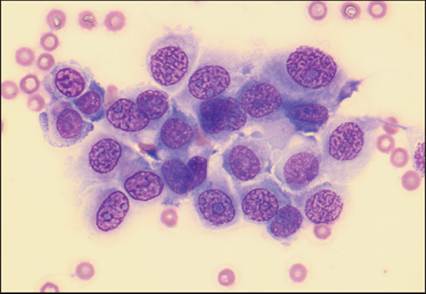
Figure 10.19 Urothelial carcinoma.
A mildly pleomorphic population of urothelial epithelial cells with increased N:C ratios. A definitive diagnosis of neoplasia could not be made from this sample. The final diagnosis was made with a surgical biopsy (modified Wright’s, 600? magnification).
When cytology is equivocal, additional testing can be recommended. Histopathologic examination is an option for these situations, but biopsy is an invasive procedure and the bladder is a difficult location to sample. Alternatively, non-invasive BRAF testing is available for suspected canine UCs with 75% of these tumors reportedly positive for the BRAF mutation (Mochizuki et al., 2015). The BRAF test is currently only commercially available on urine samples so neoplastic cells must be shed in urine for testing to occur. The BRAF mutation has (thus far) not been detected in any non-neoplastic urinary or prostatic disease, so the specificity of a positive result is reportedly 100% (Mochizuki et al., 2015; Grassinger et al., 2019).
UCs that display significant pleomorphism can be definitively diagnosed cytologically. Cells from these tumors display marked anisocytosis, moderate anisokaryosis, frequent binucleation, rare multinucleation, multiple and prominent nucleoli, and occasional mitotic figures (Figures 10.20a, b). Large, round eosinophilic globules, known as Melamed-Wolinska bodies, are observed in the cytoplasm of some neoplastic urothelial cells (Figure 10.21). These inclusions are most associated with neoplastic urothelial cells but similar inclusions, which may have variable composition, have also been noted in other normal, degenerating, and neoplastic populations (e.g. mammary carcinoma) (Arya et al., 2011; Marin et al., 2023).
Figures 10.20a,b Urothelial carcinoma. A pleomorphic variation of this tumor displaying marked anisocytosis, anisokaryosis, and multinucleation (modified Wright’s: a, 400? magnification; b, 600? magnification).
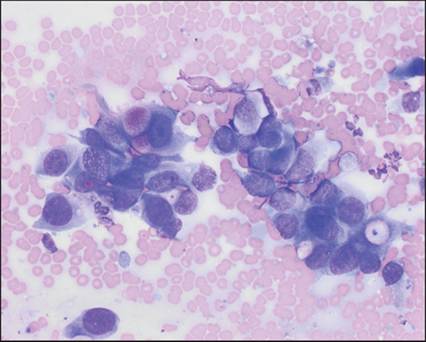
Figure 10.21 Urothelial carcinoma. Variably sized bright eosinophilic globules (Melamed-Wolinska bodies) are found in the cytoplasm of these neoplastic urothelial cells (modified Wright’s, 500? magnification).
Other neoplastic diseases are rare in the bladder, and include SCC, lymphoma, leiomyosarcoma, and rhabdomyosarcoma (Knapp & McMillan, 2010).
Hyperplasia
Chronic irritation of the bladder wall can result in significant benign urothelial epithelial hyperplasia. The most common causes of chronic irritation are urinary tract infections and urinary calculi (Martinez et al., 2003). The resulting hyperplasia can result in wall thickening and even mass-like, polypoid proliferations (polypoid cystitis).
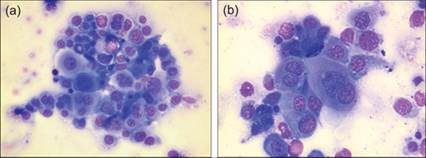
Cytologically, hyperplastic urothelial cells may display many features suggestive of well-differentiated neoplasia. Increased basophilia, moderate anisocytosis, and binucleation are common findings (Figures 10.22a, b). Depending on the cause of the hyperplasia, concurrent inflammation or infection may also be noted.
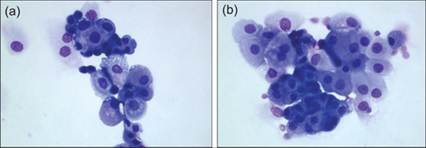
Figures 10.22a,b Hyperplastic urothelial epithelium in a dog. This dog presented for uroliths and a thickened bladder wall. Biopsy of the bladder wall confirmed a benign hyperplastic epithelium (modified Wright’s, 400? magnification).
Differentiating polypoid cystitis from UC in dogs can be a difficult process; many of the presenting signs are similar and there is cytologic overlap between the two conditions. Nuclear features of malignancy (macronuclei, abnormal nuclei, atypical mitoses, multinucleation, nuclear molding) are more suggestive of neoplastic disease and should rarely, if at all, be seen in hyperplastic lesions (Pierini et al., 2022). One should be extremely cautious when attempting to diagnose UC when there is concurrent inflammation in the sample. A thorough history investigating recurrent urinary tract infections and uroliths should be taken. Abdominal ultrasound can provide relevant information; UC usually arises in the trigone region while polypoid cystitis tends to arise in the cranioventral region. Ultimately, additional testing such as histopathology and/or BRAF testing is often required to reach a diagnosis in equivocal cases.