Inflammation
When evaluating renal cytology samples for inflammation, the amount of blood contamination must be considered. An inflammatory process can be detected when the number or proportion of leukocytes exceeds that expected from blood contamination.
Finding leukocytes in aggregates or associated with epithelium, as well as finding leukocytes that are not associated with peripheral blood (e.g. plasma cells, macrophages), provides additional support for an inflammatory process.Bacterial pyelonephritis typically results from an ascending infection, although hematogenous spread is also possible. Most diagnoses are made via urinalysis and urine culture, instead of direct renal aspiration. If aspirated, samples from pyelonephritis are expected to contain increased numbers of neutrophils, potentially with a degenerate morphology (Figure 10.5). Variable numbers of bacteria may be found. A background population of renal tubular epithelial cells and a few glomeruli may also be observed.
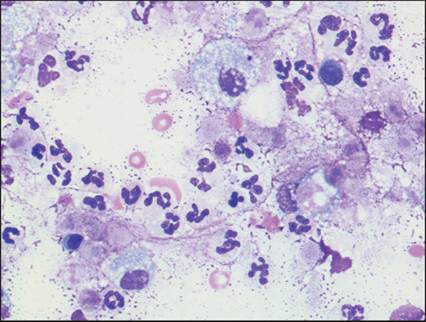
Figure 10.5 Pyelonephritis in a dog. Many neutrophils with fewer foamy macrophages. An etiology was not identified (modified Wright’s, 600? magnification).
Rarely, pyelonephritis is caused by fungal or other nonbacterial organisms and is only one symptom of systemic disease (Newman et al., 2003; Pressler et al., 2005). The type of inflammation varies with the causative agent but neutrophils often predominate. Macrophages, including epithelioid and multinucleated giant forms, often accompany fungal infections to produce pyogranulomatous inflammation.
Feline infectious peritonitis may be accompanied by nodular renal lesions (Giordano et al., 2005). Aspirates from affected kidneys often reveal normal renal elements (tubular epithelial cells and glomeruli) with a mixed population of nondegenerate neutrophils and macrophages.
Fewer lymphocytes and plasma cells may also be observed.Lymphocytic–plasmacytic inflammation is commonly associated with interstitial nephritis and chronic kidney disease (Figure 10.6). The cause of chronic interstitial nephritis is usually not apparent (microscopically or clinically).
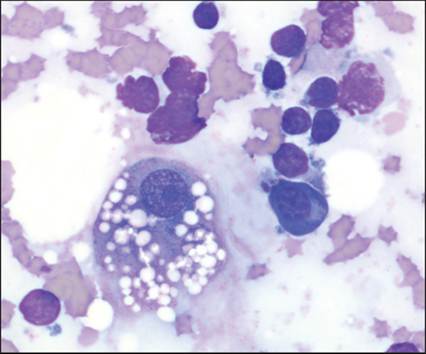
Figure 10.6 Lymphocytic–plasmacytic inflammation in a cat. Several small lymphocytes and a plasma cell associated with a lipid-laden renal tubular epithelial cell (modified Wright’s, 1,000? magnification).
Neoplasia
A variety of neoplasms affect the kidneys of small animals. Renal carcinoma arises from renal tubular epithelial cells and is the most common primary renal neoplasm of both dogs and cats (Henry, 1999; Bryan et al., 2006). Other carcinomas (urothelial, squamous, and metastatic) are rare (Meuten, 2002). Renal lymphoma can arise as a seemingly isolated lesion, most notably in cats, or as part of multicentric disease (Mooney et al., 1987). Mesenchymal neoplasms, both primary and metastatic, can also affect the kidneys, including hemangiosarcoma, fibrosarcoma, osteosarcoma, chondrosarcoma, and histiocytic sarcoma (Hahn et al., 1997; Affolter Moore, 2002; Munday et al., 2004; Bryan et al., 2006). Nephroblastoma, a mixed tumor of embryonal origin, has also been reported and may occur in very young patients (Baskin De Paoli, 1977). Most renal neoplasms are unilateral but renal carcinomas and lymphoma can be bilateral. Most renal neoplasms are malignant. Benign tumors (adenoma, papilloma, fibroma) are rare, small (2 cm), and usually an incidental finding at necropsy (pale cortical nodule in an otherwise grossly normal kidney; Baskin De Paoli, 1977).
Aspirates from renal carcinoma are moderately to highly cellular. The epithelial cells have moderately to deeply basophilic cytoplasm and typically occur in cohesive clusters, sheets, and, rarely, acini (Figure 10.7).
Cells within clusters are often tightly packed and jumbled, with irregular nuclear spacing and indistinct cell borders. In fewer tumors, the cells may be individualized and round (Figure 10.8). Nuclear to cytoplasmic (N:C) ratios are variable but are often increased above normal. Some renal carcinomas are monomorphic in appearance. Others display moderate anisocytosis and anisokaryosis with bi- and multinucleation (Figure 10.9). 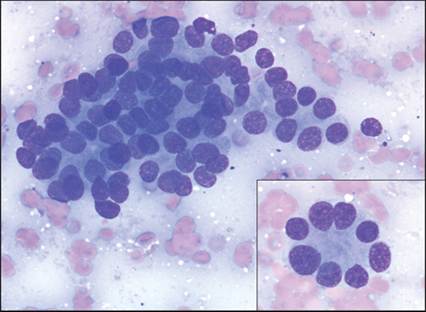
Figure 10.7 Renal carcinoma in a dog. A disorganized cluster of neoplastic epithelial cells with indistinct cell borders. Inset: acinar formation from the same tumor (modified Wright’s, 600? magnification).
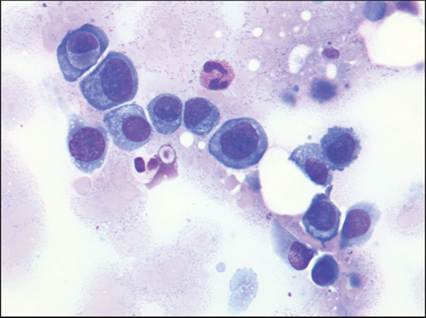
Figure 10.8 Renal carcinoma in a cat. Most of the neoplastic epithelial cells in this sample were individualized and round (modified Wright’s, 600? magnification).
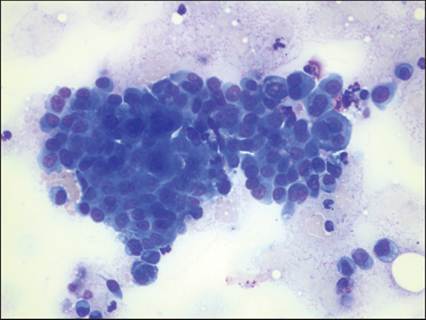
Figure 10.9 Renal carcinoma in a cat. A pleomorphic neoplastic population displaying anisocytosis, anisokaryosis, and multinucleation (modified Wright’s, 400? magnification).
Urothelial carcinomas (UCs), also known as transitional cell carcinoma (TCC), of the kidney are morphologically similar to those described later for the urinary bladder. Squamous cell carcinomas are rare and comparable to squamous cell carcinoma in cutaneous and other locations (see Chapter 4). Metastatic carcinomas are also rare and the tissue of origin is often not obvious from cytology alone. Pertinent history and knowledge of the primary neoplasm can help identify the tumor in such cases (Figure 10.10).
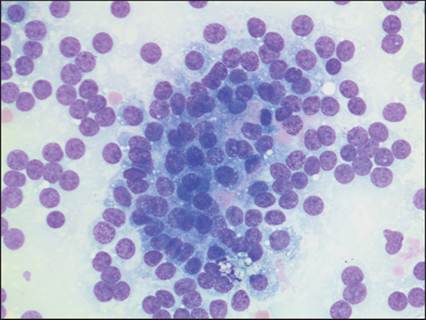
Figure 10.10 Metastatic thyroid carcinoma in a dog.
A loosely cohesive epithelial population with many free nuclei suggestive of a neuroendocrine origin. A primary thyroid carcinoma with multiple metastatic lesions was identified at necropsy (modified Wright’s, 600? magnification).
Aspirates of renal lymphoma are often highly cellular and will appear cytologically like lymphoma aspirates in lymphoid and other tissues (see Chapter 5). A homogeneous population of large lymphocytes with finely stippled chromatin will be present, possibly along with a few normal renal elements (Figure 10.11). Neoplastic lymphocytes from renal lymphoma rarely exfoliate into the urine and can be noted on a urine sediment exam (Witschen et al., 2020). Differentiation between neoplastic and inflammatory lymphoid populations is usually straightforward in renal aspirates. Lymphoma aspirates tend to be highly cellular with a homogeneous population of large cells. Inflammatory lymphoid populations are typically less cellular, more heterogeneous, and composed of small lymphocytes with plasma cells.
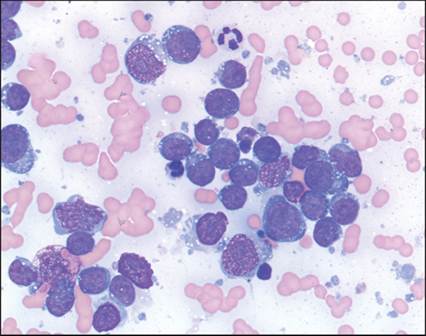
Figure 10.11 Renal lymphoma in a cat. A homogeneous population of large lymphocytes with high N:C ratios, finely stippled chromatin, and occasional nucleoli (modified Wright’s, 600? magnification).
Many renal mesenchymal neoplasms aspirate poorly (fibrosarcoma) or are markedly contaminated by blood (hemangiosarcoma) and rarely provide diagnostic samples for cytology. Some sarcomas, such as chondrosarcoma and osteosarcoma, may produce more cellular aspirates, but are rare metastatic lesions (Figures 10.12, 10.13). Histiocytic sarcoma can affect the kidneys as part of disseminated disease and aspirates are typically highly cellular, containing a pleomorphic population of individual round to spindle-shaped cells (Figures 10.14a, b). These cells have lightly basophilic cytoplasm and often contain a few small, distinct, clear vacuoles.
Marked anisocytosis and anisokaryosis are typically evident, along with frequent bi- and multinucleation.Nephroblastomas have a ‘triphasic’ pattern of epithelium, mesenchyme, and embryonic glomeruli that can be seen histologically, but all three features are rarely observed cytologically. More commonly, aspirates contain only poorly differentiated, loosely cohesive epithelial cells with lightly basophilic cytoplasm, high N:C ratios, round nuclei, and finely stippled chromatin (Neel & Dean, 2000). These poorly differentiated epithelial cells can be mistaken for large lymphocytes; however, rare cohesion, particularly rosette formation, will help suggest the true diagnosis (Figure 10.15). Small spindle cells with dark nuclei, representing the mesenchymal component of the tumor, may also be present. Glomerular structures are rare (de Lorenzi et al., 2007).
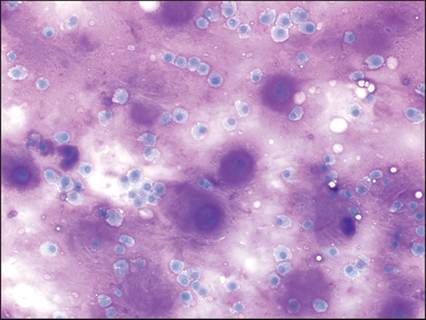
Figure 10.12 Metastatic chondrosarcoma. A large amount of extracellular matrix and cells occasionally embedded within chondroid lacunae are characteristic of this tumor (Modified Wright’s, 200? magnification).
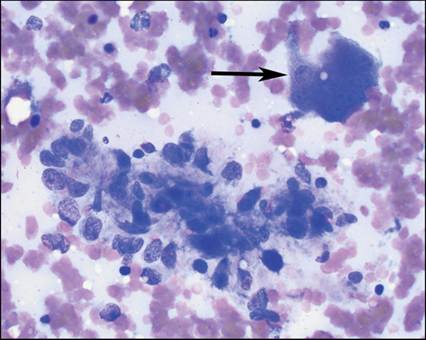
Figure 10.13 Metastatic osteosarcoma in a dog displaying an aggregate of neoplastic osteoblasts and a multinucleated osteoclast (arrow). Rare tubules of epithelium were also noted to confirm a renal origin (modified Wright’s, 500? magnification).
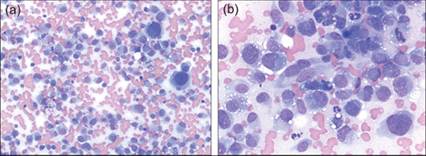
Figures 10.14a,b Histiocytic sarcoma in a dog with disseminated disease. (a) 200? magnification view displaying high cellularity and marked pleomorphism. (b) 600? magnification displaying round to spindle-shaped cells with lightly basophilic cytoplasm and small vacuoles (modified Wright’s).
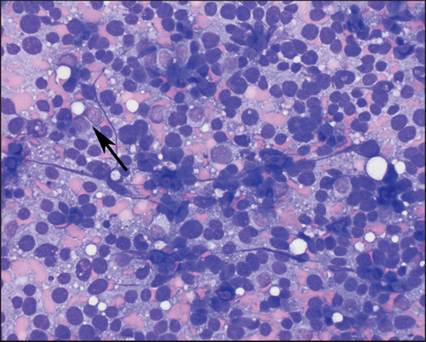
Figure 10.15 Nephroblastoma (presumed).
A retroperitoneal mass in a young dog contains many free nuclei and poorly differentiated cells that could be mistaken for a lymphoid origin, but rare cohesive cells (arrow) suggest an epithelial origin. In this location, a nephroblastoma is presumed but the cytology alone is similar to other primitive neuroectodermal tumors (modified Wright’s, 500? magnification).
Other renal abnormalities
Renal and perirenal cysts may be congenital or acquired and can present as single or multiple lesions. Aspirates of cysts produce a clear fluid with low cellularity. The few nucleated cells present are predominantly foamy macrophages. A few monomorphic epithelial lining cells may also be observed. Renal carcinomas can have cystic regions that mimic benign cysts. If underlying neoplasia is suspected, additional aspirates or biopsy of the suspicious tissue should be performed.
Hydronephrosis is a fluid-filled dilation of the renal pelvis due to obstructed urine flow. Diagnosis is usually made via ultrasonography. Aspirates from hydronephrotic kidneys will contain poorly cellular, watery fluid with a creatinine concentration higher than peripheral blood, consistent with urine.