Urinary sediment
Sampling, preparation, and evaluation
Urine sediment examination is typically part of a complete urinalysis. The basics of sediment preparation are detailed in the following paragraphs (Osborne & Stevens, 1999; Gunn-Christie et al., 2012).
Examination of the sediment can identify various inflammatory, infectious, hemorrhagic, and metabolic processes in the patient. Neoplastic cells from prostatic and bladder tumors may also be observed in urine sediment, but this sample is not recommended for diagnosing neoplasia. Direct sampling of the suspected neoplasm, via FNA or traumatic catheterization, is recommended to obtain a higher quality sample for cytology.Urine can be obtained via voided (free-catch), catheterization, or cystocentesis methods. Free-catch collection is a non-invasive process that is easy to perform, but these voided samples are prone to contamination with genital and skin elements. Catheterization is minimally invasive but could introduce infection and is still susceptible to external contamination. Catheterized samples often have higher numbers of urothelial cells, and these cells can be found in clusters. Cystocentesis is the most invasive method and can be complicated by iatrogenic hemorrhage or enterocentesis (Garner et al., 2011). However, cystocentesis samples avoid contamination by the genital tract and are considered the best samples for urine culture.
A sterile container or plain blood collection tube is recommended for sample submission. Anticoagulants, preservatives, or clot-enhancing components can interfere with the urine dipstick reactions, sediment exam, and/or culture. To obtain the most representative results, urine should be analyzed within 30 minutes of collection. If rapid evaluation is not possible, the urine should be refrigerated. A refrigerated sample should be allowed to warm back to room temperature before being analyzed.
Urine samples should ideally be analyzed within 24 hours of collection to limit in-vitro bacterial growth, crystal formation, and cast and/or cellular degradation.To prepare a sample for microscopic examination, 5 ml of well-mixed urine is centrifuged at low speed (450 ? g) for 5 minutes. The supernatant is pipetted off, leaving 0.5 ml of fluid and sediment. In healthy patients, grossly visible sediment will not be apparent. The sediment is resuspended in the remaining fluid by gentle aspiration and discharge from a pipette. A drop of the suspension is placed on a glass slide and covered with a coverslip.
The wet mount should be examined microscopically in both a low-power field (lpf, 100? magnification) and a high-power field (hpf, 400? magnification) with lighting appropriate to unstained specimens. Lighting options for most microscopes include lowering the substage condenser or closing the iris diaphragm, both of which will increase contrast and help visualize elements. Phase contrast condensers are another option for increasing contrast but are not routinely available. Cellular, crystal, and other elements are evaluated semiquantitatively at low or high power.
New methylene blue or urine stains (e.g. Sedistain) can be added to urine sediment to improve visualization of certain urine elements, most notably hyaline and waxy casts (Figure 10.23). However, they can also introduce artifactual dilution of the sample and stain debris that can be mistaken for bacteria. An alternative method to improve identification of urine elements is to prepare and stain a dry slide of the urine. A drop of resuspended urine sediment is used to make a sediment or line preparation. Once dry, the slide can be stained with Wright’s, Diff-Quik, or Gram stain. Wright’s- or Diff-Quik®-stained dry slides can help differentiate cellular elements (erythrocyte versus leukocyte versus epithelial cell), whereas Wright’s-, Diff-Quik-, or Gram-stained slides can confirm the presence of bacteria (Swenson et al., 2011).
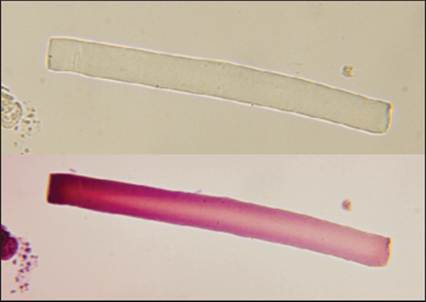
Figure 10.23 Urine sediment unstained (top) and with Sedistain (bottom). The waxy cast is easily visualized with the addition of Sedistain (400? magnification). (Courtesy Peter S. MacWilliams.)
Normal findings
Cellular elements normally found in urine include low numbers of erythrocytes, leukocytes, and epithelial cells (urothelial and/or squamous). Certain casts and crystals may also be present in low numbers, as elaborated upon in the subsequent sections. Lipid droplets are frequently encountered. Spermatozoa are expected in intact males. Abnormal findings include increased numbers of normal elements and the presence of other elements, as detailed below.
Cells
Erythrocytes are uniform in size, round or crenated in shape, and moderately refractile (shiny) in appearance (Figures 10.24a, b). They often appear colorless but may have a slight red–orange tinge (Figure 10.25). Central pallor may be visible. A few erythrocytes (0–5/hpf) are considered a normal finding. Increased numbers can be seen with uroliths, urinary tract infections, idiopathic cystitis, neoplasms, and coagulopathies. Iatrogenic hemorrhage associated with cystocentesis will also increase the number of erythrocytes.
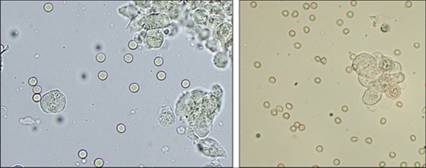
Figure 10.24a,b Many erythrocytes from a dog with hematuria secondary to urothelial carcinoma. Erythrocytes vary from round and smooth to biconcave to slightly crenated. A few larger irregular neoplastic urothelial cells are also present, found individually and in clusters (unstained, 400? magnification).
Figure 10.25 Erythrocytes with a red-orange tinge (unstained, 400? magnification).
Most leukocytes in urine are neutrophils, although they often cannot be identified as such by sediment examination.
These leukocytes will be uniform in size, round in shape, and slightly granular in appearance (Figure 10.26). They are larger than erythrocytes (1.5–2 times the size) and smaller than epithelial cells. A lobulated nucleus may rarely be visible (Figure 10.27). A few leukocytes (0–5/hpf) are considered a normal finding. Increased numbers are most associated with urinary tract infections. Sterile inflammation, associated with neoplasms or uroliths, is also possible but less common. 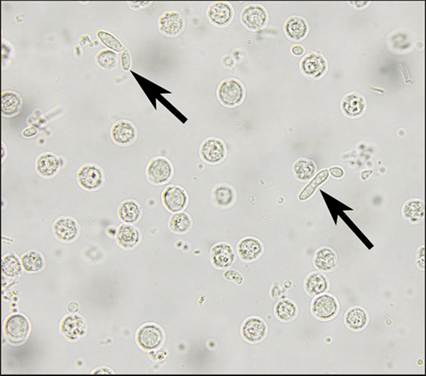
Figure 10.26 Many leukocytes (presumably neutrophils) with a diffusely granular appearance. Rare oval to elongated, budding yeast are also present (arrows) as the source of inflammation in this case (unstained, 400? magnification).
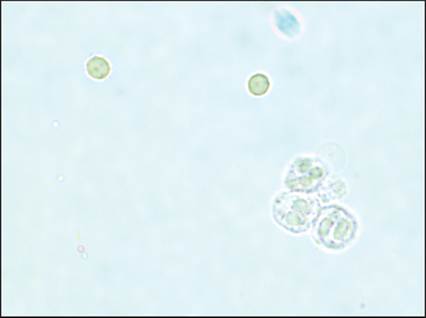
Figure 10.27 Three leukocytes with visible lobulated nuclei (neutrophils, lower right). Two red–orange erythrocytes are also present (unstained, 400? magnification).
Squamous epithelial cells in urine may originate from the skin, distal urethra, vaginal tract, or prepuce. They are large and often irregularly shaped with angular borders (Figure 10.28). They may have a small central nucleus or be anucleate. They occur singly or in sheets. Squamous cells in urine are usually the result of sample contamination and are not clinically significant. A rare exception is squamous metaplasia of the prostate (secondary to estrogen exposure) with desquamated cells found in the urine.
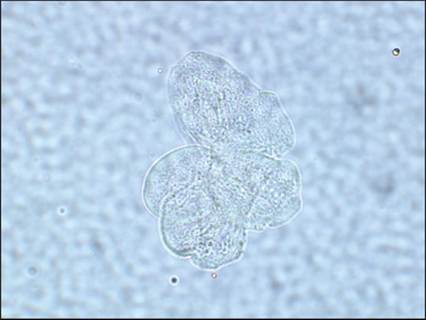
Figure 10.28 A cluster of squamous epithelial cells with irregular, angular borders (unstained, 400? magnification).
Urothelial cells (Figure 10.29) line the renal pelvis, ureter, bladder, and proximal urethra. They are slightly variable in size but consistently larger than leukocytes (2–4 times the size) and smaller than squamous cells (Figure 10.30).
They are often round to cuboidal with a slightly granular appearance. Rarely, cells will be caudate in shape, suggestive of a renal pelvic origin. They have a round, central nucleus, although it is not always visible. Urothelial cells can be found individually or in small clusters. Low numbers of urothelial cells are considered a normal finding. Catheterized samples will have increased numbers of urothelial cells as the passage of the catheter dislodges normal cells. Increased numbers will also be seen with urinary tract infections, uroliths, and UC. The cells from UC are often pleomorphic in morphology, as described for bladder cytology (Figure 10.31). In some cases of UC, cellular details will be difficult to discern with an unstained specimen. Applying Wright’s stain to a dried sediment smear may help visualize details in these cases (Figures 10.32 a, b). 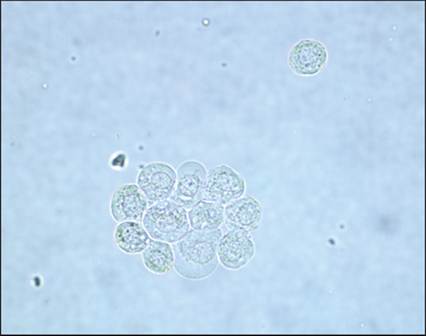
Figure 10.29 Normal urothelial cells. A small cluster and a single cell displaying mild anisocytosis. Round nuclei are occasionally visible within the cells (unstained, 400? magnification).
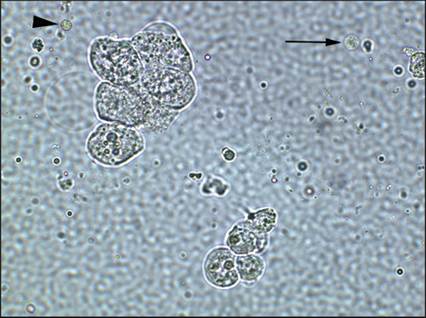
Figure 10.30 A small cluster of normal urothelial cells (bottom) with size comparisons to squamous epithelial cells (upper left), a leukocyte (arrow), and an erythrocyte (arrowhead) (unstained, 400? magnification).
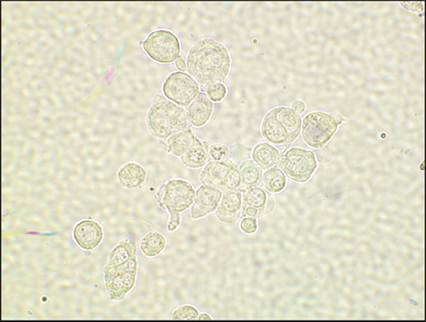
Figure 10.31 A population of neoplastic urothelial cells with moderate anisocytosis, anisokaryosis, and binucleation (unstained, 400? magnification).
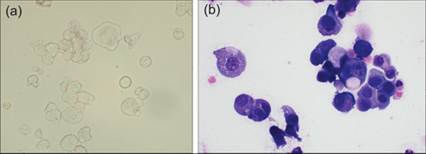
Figure 10.32a,b Urothelial carcinoma. The unstained sediment (a, 400? magnification) contains clusters of epithelial cells that vary in size and are suspicious for neoplasia, but additional cellular details are difficult to visualize.
A stained specimen (b) further displays anisokaryosis and binucleation to support the diagnosis of neoplasia (modified Wright’s, 500? magnification).
Renal epithelial cells line the renal tubules of the kidney. They are smaller than urothelial cells but slightly larger than leukocytes. Like urothelial cells, they are round to cuboidal in shape, have a round nucleus, and can be found individually or in clusters. As such, it is very difficult to accurately differentiate them from small urothelial cells. Renal epithelial cells are rarely found and definitively identified in urine. When present, they suggest renal tubular disease.
Casts
Casts are cylindrical molds of renal tubules composed of mucoproteins and, often, cellular elements. Casts are variable in length but all have parallel sides and are approximately 3–4 leukocytes in width. Casts do not preserve well in urine sediment; they easily fragment into short pieces, making identification difficult. Also complicating identification is the fact that mucus strands, fibers, and aggregates of debris sometimes mimic casts.
Hyaline casts are composed of protein only. They are very faint (almost transparent) and homogeneous with rounded ends (Figure 10.33). A low number of hyaline casts is a normal finding. Increased numbers can be seen with proteinuria, glomerular disease, and renal tubular damage. Cellular casts contain intact renal tubular epithelial cells embedded within a glycoprotein matrix (Figure 10.34). Rarely, entire segments of intact tubules will slough (Figure 10.35). Both forms are an abnormal finding and indicate renal tubular damage. Granular casts may result from the breakdown of cellular casts or the precipitation of proteins. They vary from finely to coarsely granular in appearance, with no intact cells (Figure 10.36). Low numbers of granular casts are considered a normal finding. Increased numbers are associated with renal tubular damage and may accompany cellular casts and/or waxy casts. Waxy casts are the presumed final breakdown product of cellular and granular casts. They are faint, smooth, and wide with blunt ends (Figure 10.37). They are an uncommon finding and thought to indicate chronic renal tubular disease. Multiple types of casts and mixed casts can be observed in a single urine sample (Figures 10.38, 10.39).
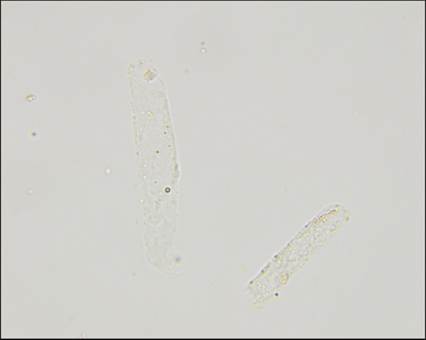
Figure 10.33 Two faint hyaline casts with parallel walls and rounded ends (unstained, 400? magnification).
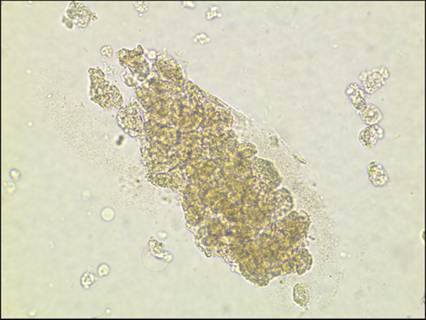
Figure 10.34 Cellular cast. Outlines of tubular epithelial cells are discernible in a cylindrical form (unstained, 400? magnification).

Figure 10.35 An intact fragment of renal tubule that sloughed during acute tubular injury (unstained, 400? magnification).

Figure 10.36 Granular cast. Variably sized fat droplets are adhered to the surface (unstained, 400? magnification).
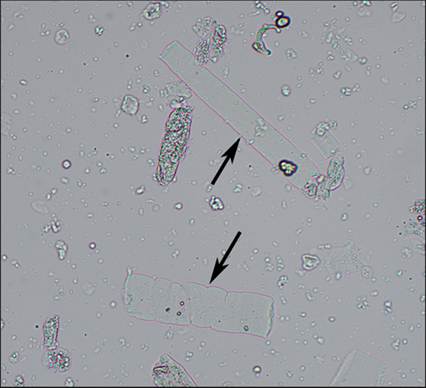
Figure 10.37 Two waxy casts (arrows) with blunt ends (unstained, 400? magnification).
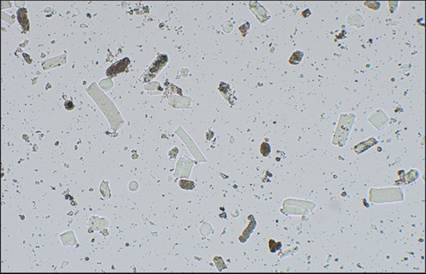
Figure 10.38 Multiple casts (granular, waxy, and mixed) in a dog with severe acute kidney injury (unstained, 100? magnification).

Figure 10.39 Mixed cast. Although most of the cast is homogeneous (waxy), there is some granularity visible at the lower end (unstained, 400? magnification). (Courtesy Kristen R. Friedrichs.)
Rarely, other cells or elements that are present in the renal tubules can become trapped within a mucoprotein matrix, creating unique casts. The significance of the cast varies with the embedded material. Leukocyte casts indicate renal inflammation while erythrocyte casts indicate renal hemorrhage. Hemoglobin casts indicate intravascular hemolysis and subsequent hemoglobinuria (Figure 10.40). Myoglobin casts indicate severe muscle damage and subsequent myoglobinuria. Bilirubin casts could be associated with any cause of conjugated hyperbilirubinemia and bilirubinuria. Bacterial casts have been reported with bacterial pyelonephritis (Phelps et al., 2022) and amorphous crystalline casts have been reported in a dog with massive uric acid crystalluria (Tvedten et al., 2019).
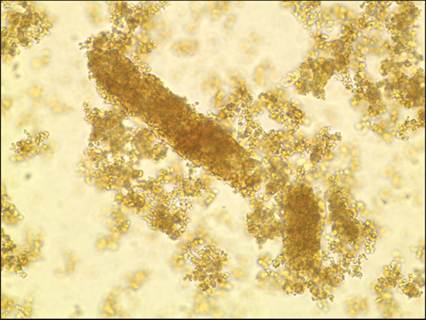
Figure 10.40 A fragmented hemoglobin cast from a dog with intravascular hemolysis (unstained, 400? magnification).
Crystals
Some crystals are considered a normal finding in low or moderate numbers while other crystals are considered an abnormal finding at any number. Large numbers of any crystal are considered a risk for, but not definitive evidence of, urolith formation. Fresh urine is the best sample to evaluate for crystals. Refrigeration and storage can both enhance in-vitro crystal formation, making accurate interpretation difficult.
Magnesium ammonium phosphate (a.k.a. struvite or triple phosphate) crystals are colorless, variably sized crystals that are often rectangular in shape with a three-to-six-sided ‘coffin-lid’ appearance (Figure 10.41). In cats, struvite crystals may have fewer sides and lack the coffin-lid morphology (Figure 10.42). Struvite crystals are typically found in alkaline urine and can be seen in healthy animals and animals with uroliths. Struvite crystals can also form in patients with urinary tract infections if those infections raise the urine pH.

Figure 10.41 Struvite crystals in a dog with the classic ‘coffin-lid’ appearance (unstained, 250? magnification).
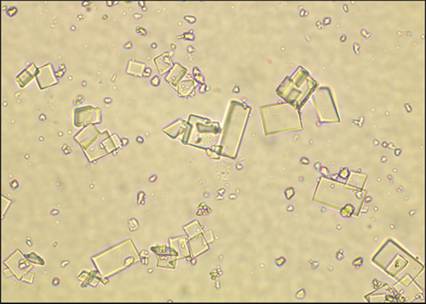
Figure 10.42 Struvite crystals in cats do not always have the classic ‘coffin-lid’ appearance (unstained, 400? magnification).
Calcium oxalate dihydrate crystals appear as colorless, variably sized squares with intersecting diagonal lines (envelope shape; Figure 10.43). They are considered a normal finding in low to moderate numbers and can also form in vitro with storage. Larger numbers may be associated with uroliths.
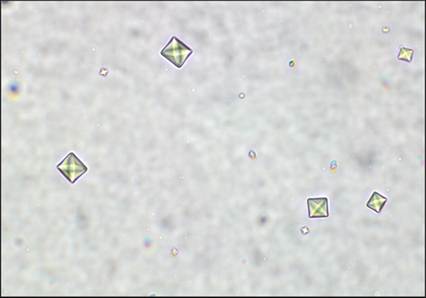
Figure 10.43 Calcium oxalate dihydrate crystals with intersecting diagonal lines (envelope shape) (unstained, 400? magnification).
Calcium oxalate monohydrate crystals vary in size and shape. Possible shapes include rectangles with pointed ends (picket fence), ovals (hemp seed), spindles, and dumb-bell forms (Figures 10.44, 10.45). Large numbers of these crystals are often observed with ethylene glycol toxicosis. The significance of lower numbers is uncertain; they may be a normal or non-specific finding, although even low numbers of the picket fence morphology should raise concern for ethylene glycol toxicity.
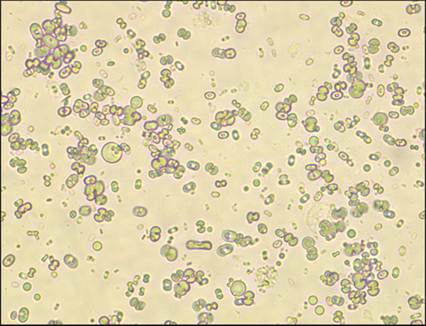
Figure 10.44 A low-power view demonstrating the pleomorphic nature of calcium oxalate monohydrate crystals (unstained, 400? magnification).
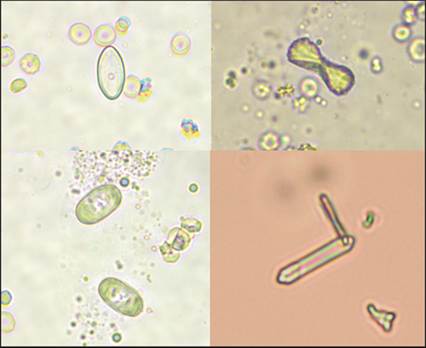
Figure 10.45 Closer view of the variable forms of calcium oxalate monohydrate crystals (unstained, 400? magnification). (Lower right courtesy Anne Barger.)
Bilirubin crystals are small golden-brown to red needles or granules that are often found in aggregates (Figure 10.46). They are occasionally associated with a fat droplet on one end, giving them a flashlight appearance. A few bilirubin crystals may be found in concentrated urine of normal dogs. Increased numbers indicate conjugated hyperbilirubinemia with subsequent bilirubinuria.

Figure 10.46 Small, red-brown, needle-shaped bilirubin crystals (unstained, 400? magnification).
Ammonium biurate crystals are golden-brown spheres that often have irregular thorn-like protrusions (Figure 10.47). Smooth forms (lacking thorn-like protrusions) are less commonly seen (Figure 10.48). In most patients, ammonium biurate crystals are an abnormal finding indicating hepatic failure or portosystemic shunting. A few canine breeds, especially Dalmatians, form these crystals as part of a congenital defect in uric acid metabolism. These dogs may also form uric acid crystals, colorless blunted diamonds, or ovals that often aggregate into rosettes (Figure 10.49).

Figure 10.47 Ammonium biurate crystals with irregular surface spicules (thorn-apple morphology) (unstained, 400? magnification).
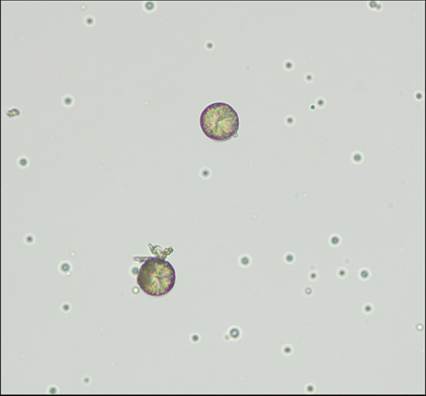
Figure 10.48 Round ammonium biurate crystals with a predominantly smooth surface (unstained, 400? magnification).

Figure 10.49 Uric acid crystal with a pointed oval/blunted diamond shape (unstained, 400? magnification). (Courtesy Ruth A. Houseright.)
Cystine crystals are colorless, hexagonal crystals that often aggregate into layers (Figure 10.50). They are an abnormal finding seen in patients with acquired or congenital defects in urinary cysteine reabsorption.
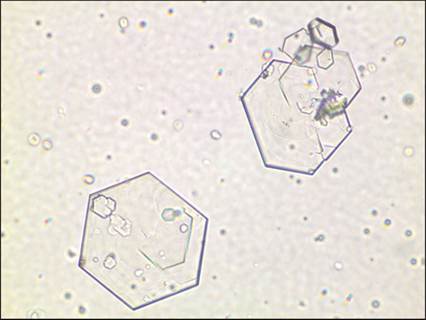
Figure 10.50 Hexagonal cystine crystals (unstained, 400? magnification).
Amorphous crystals are lightly colored, refractile granules that form variably sized aggregates (Figure 10.51). Such aggregates can be mistaken for colonies of cocci bacteria. Amorphous crystals will be more variable in size and more refractile than bacteria, but a stained slide of sediment should be examined if there is any doubt regarding identity. These crystals may be urates or phosphates in origin and their significance is often unclear.
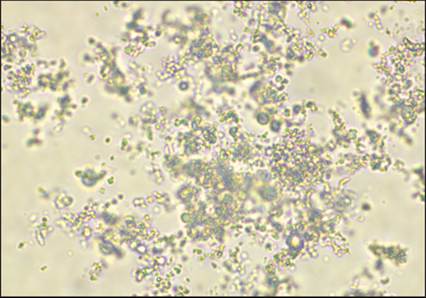
Figure 10.51 An aggregate of amorphous crystals. Their high refractility helps distinguish them from debris and bacteria (unstained, 400? magnification).
Certain medications, including ampicillin, sulfadiazine, and ciprofloxacin, and radiographic contrast agents can precipitate in urine and produce variably shaped crystals (Figure 10.52). Fan-like aggregates and bundles of rectangular crystals have been reported, but the exact morphology of these crystals is hard to predict in veterinary medicine (Escobar & Grindem, 2010).

Figure 10.52 Fan-like aggregates of crystals in a dog receiving multiple antibiotics (unstained, 400? magnification).
Other crystals are rarely reported in veterinary medicine and often have an uncertain significance. Calcium phosphate forms long, thin, colorless, rectangular crystals that often aggregate (Figure 10.53). Cholesterol crystals are flat, colorless rectangles (often with a notched corner). Xanthine crystals are morphologically identical to ammonium biurate crystals (Davis & Grindem, 2015). They are rarely reported and have a distinct association with allopurinol administration.
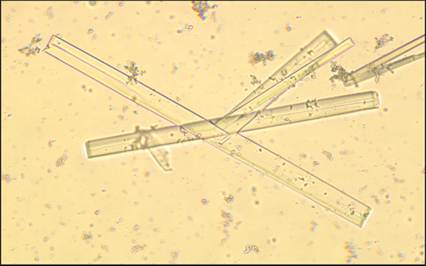
Figure 10.53 Suspect calcium phosphate crystals (unstained, 400? magnification).
When crystals cannot be identified by routine sediment examination, dissolution studies may help better characterize their origin. One drop of urine sediment is mixed with one drop of a specific chemical, and the sediment is re-examined to determine whether the crystals are soluble or insoluble with that chemical. The process is repeated with additional chemicals and/or heat, and the combination of results can sometimes assist in crystal identification (Figure 10.54). However, dissolution results are only known for common crystals, and some discrepant results have been reported (Table 10.1) (Lee et al., 2022; Thompson, 1981).

Figure 10.54 Oval (hemp seed) crystals in a cat. Morphology is suggestive of calcium oxalate monohydrate but difficult to confirm in isolation. Dissolution studies revealed the crystals to be soluble in hydrochloric acid, insoluble in acetic acid, and partially soluble in sodium hydroxide, results further consistent with a calcium oxalate origin (unstained, 400? magnification).
Table 10.1 Dissolution results for common crystals
| Crystal | Soluble with | Insoluble with | Discrepant results | Notes |
| Calcium oxalate | HCl | AA | NaOH, heat | |
| Calcium carbonate | HCl, AA | NaOH, heat | CO2 gas produced when dissolving with HCl or AA | |
| Triple phosphate | HCl, AA | NaOH, heat | ||
| Calcium phosphate | HCl, AA | NaOH, heat | ||
| Amorphous phosphate | HCl, AA | NaOH, heat | ||
| Amorphous urate | NaOH, heat | HCl, AA | May dissolve in HCl or AA to produce uric acid | |
| Ammonium biurate | HCl, AA, NaOH, heat | Ammonia gas produced when dissolved with NaOH. HCl or AA dissolve crystals slowly to form uric acid | ||
| Uric acid | NaOH | HCl, AA | Heat | |
| Cystine | NaOH, HCl | AA, heat | ||
| Bilirubin | HCl, AA, NaOH | Heat | ||
| HCl = 30% hydrochloric acid, AA = 30% acetic acid, NaOH = 10% sodium hydroxide, heat = 60° Celsius. | ||||
| Note: 10% potassium hydroxide (KOH) can be substituted for NaOH with equivalent results. | ||||
Organisms
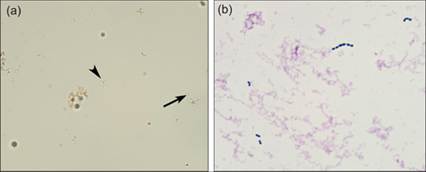
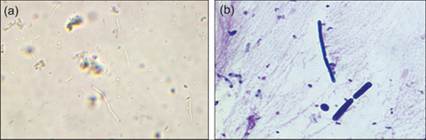
Bacteria are small and refractile in appearance on wet mount preparations. Rods are the easiest form to identify, especially in large numbers, because their shape is unique (Figure 10.55). Fewer rods can be difficult to identify definitively. Cocci and small pleomorphic organisms are more difficult to identify overall and can be confused with debris or amorphous crystals (Myers et al., 2022). If cocci or low numbers of rods are suspected, preparation of a dry slide stained with Gram, Wright’s, or Diff-Quik stain is recommended for confirmation (Figures 10.56a, b and 10.57a, b). The significance of bacteriuria varies with the method of collection, type of bacteria, and host response. Free-catch samples are easily contaminated with a mixed population of mucocutaneous bacteria. Catheterized samples are less susceptible to contamination, but it can still occur. Bacteria in cystocentesis samples are considered pathologic unless accidental enterocentesis has occurred (Figures 10.58a, b). With all collection methods, true infection is expected to be accompanied by an inflammatory response, unless the patient is immunocompromised by neutropenia, steroids, chemotherapy, hyperadrenocorticism, or other disease.

Figure 10.55 Large numbers of bacterial rods can usually be identified in wet preparations. Also present is a section of fungal hyphae (upper right) and a single struvite crystal (lower left) (unstained, 500? magnification).
Yeast and fungal organisms are rarely observed in urine samples. Yeast are round to oval structures that may display budding. Low numbers of certain yeasts (e.g. Candida, Malassezia) may be the result of contamination, especially if the sample was voided. Low numbers of other yeasts (e.g. Blastomyces, Cryptococcus) indicate true infection, often associated with systemic disease (Brandt & Blauvelt, 2010). High numbers of any yeast indicate true infection, which can arise as a primary disease or secondary to immunosuppression or chronic antibiotic usage, depending on the organism. Fungal hyphae are long branching structures with parallel walls and occasional septations (Figure 10.59). Any fungal hyphae in urine are presumed pathogenic, although environmental contamination should also be considered in voided samples.
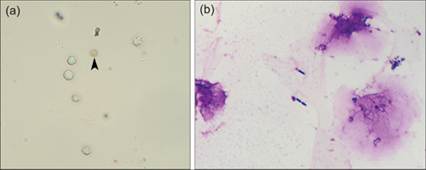
Figure 10.56a,b (a) A few leukocytes, one crenated erythrocyte (arrowhead) and low numbers of rod bacteria (unstained, 400? magnification). (b) A stained specimen confirms the rod bacteria (modified Wright’s, 500? magnification).
Figures 10.57a,b (a) Bacterial cocci can be difficult to identify in wet preparations, being mistaken for debris or amorphous crystals. Pairs (arrow) and chains (arrowhead) of organisms can help with identification (unstained, 400? magnification). (b) Modified Wright’s stain of the same specimen, confirming the presence of cocci (1,000? magnification).
Figures 10.58a,b Fecal contamination. A mixed population of bacteria with no inflammatory reaction (a: unstained, 400? magnification; b: modified Wright’s, 1,000? magnification).

Figure 10.59 Branching fungal hyphae (unstained, 500? magnification).
Parasite eggs are rare findings in urine samples, including those from the kidney worm, Dioctophyma renale (Vieira et al., 2011), and bladder worm, Pearsonema plica (Figure 10.60). Gastrointestinal parasite eggs may also be seen in urine contaminated with feces.

Figure 10.60 Pearsonema plica egg (unstained, 500? magnification).
Other elements
Lipid droplets are small, variably sized, and highly refractile (Figure 10.61). They must be differentiated from erythrocytes, which will be uniform in size. In addition, lipid droplets float under the coverslip and will often focus on a different plane than other urine elements. Mucus often comes in a cylindrical form and can easily be mistaken for a cast. Whereas casts will be uniform in width, mucus threads will vary in width and often have an irregular shape with tapered ends (Figure 10.62). Fibers can also be mistaken for casts but are typically larger and contain an internal structure suggesting a processed origin (Figure 10.63). Glove powder (Figure 10.64) contains corn starch, which could be mistaken for a urinary crystal. Glass shards (from slides or coverslips) are irregular refractile fragments that could also be mistaken for a crystal but are more variable in appearance (Figure 10.65). Multiple types of pollen may be encountered in urine sediment. They are variable in size and shape but typically quite large and golden-brown (Figure 10.66). Sperm are easy to identify, with a characteristic appearance including a pointed head and long tail (Figure 10.67).
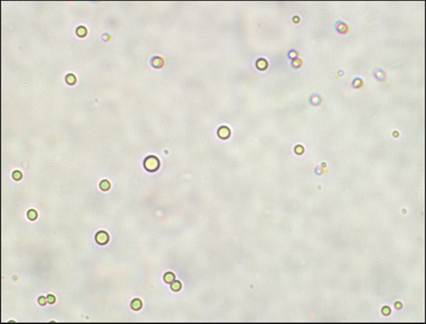
Figure 10.61 Variably sized and highly refractive lipid droplets (unstained, 400? magnification).

Figure 10.62 Mucus. The irregular borders help differentiate mucus threads from casts (unstained, 400? magnification).

Figure 10.63 A large textile fiber (unstained, 200? magnification).

Figure 10.64 Starch (glove powder) granules (unstained, 400? magnification).
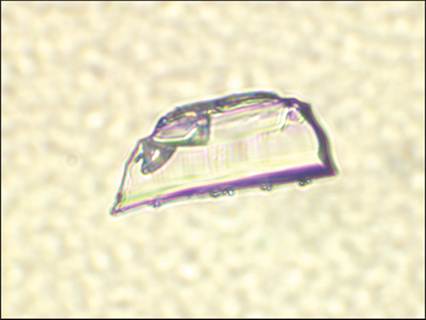
Figure 10.65 Glass shard. The irregular shape helps differentiate this from a urinary crystal (unstained, 400? magnification).
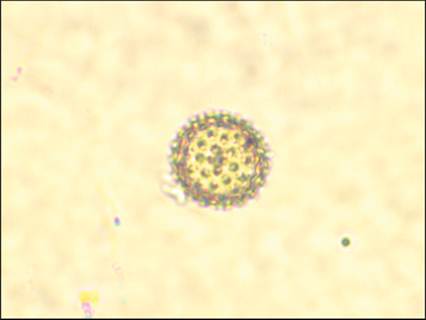
Figure 10.66 A spiculated pollen granule (unstained, 400? magnification).

Figure 10.67 Sperm from the urinalysis of an intact male dog (unstained, 400? magnification).