Bone
Sampling
While obtaining a bone aspirate of diagnostic cellularity can be challenging, the benefits of bypassing a more involved bone biopsy are valuable if a sample of diagnostic cellularity can be obtained.
Aspirates of lytic or proliferative bone lesions are less invasive than biopsy, and histopathology of bone requires additional time for the decalcification process required prior to standard processing. Poorly exfoliative lesions or those with considerable peripheral blood contamination may require biopsy for diagnosis. Aspiration or fenestration is performed with an 18–22-gauge needle. Using a smaller gauge needle risks collecting a poorly cellular, nondiagnostic sample but may be more appropriate in lesions with considerable bone lysis or smaller patients to avoid iatrogenic trauma. Sampling at the periphery of a lesion can result in high numbers of reactive osteoblasts, which may preclude accurate diagnosis of the primary pathology. Peripheral blood contamination is a common problem, and discontinuation of negative pressure on the syringe when blood enters the needle hub may help limit the amount of background blood.Normal cytology
Bone cytology samples are often of low cellularity and primarily consist of peripheral blood. Healthy bone is not expected to exfoliate well on cytology. Bone aspirates are typically performed on lesions observed on radiographs (lysis, proliferation) or palpable masses or abnormalities noted on physical examination. Consequently, the expectation of exfoliation on aspiration is greater than normal due to the presence of pathologic change. In a study of 36 lytic, proliferative, or lytic and proliferative bone lesions aspirated via ultrasound guidance, diagnostic samples were obtained in 32 cases (Britt et al., 2007).
Reactive bone
A significant complicating feature of aspirating bone lesions is the exfoliation of nonneoplastic reactive osteoblasts into a sample, either in place of or in concert with inflammatory or neoplastic cells.
Reactive osteoblasts are typically rounded or ovoid in shape and have a plasmacytoid or ‘flag’ appearance, with a round, eccentric nucleus and polarized cytoplasm (Figure 12.12). The cytoplasm is expected to be moderately basophilic and moderate to abundant in amount, and perinuclear clearing, consistent with a prominent Golgi apparatus, may be appreciated. The cells may contain variable numbers of fine, azurophilic granules within the cytoplasm. The chromatin pattern is generally finely to coarsely stippled, and nucleoli are often indistinct or absent; however, observation of nucleoli is not pathognomonic for neoplastic cells. Reactive osteoblasts often display mild to moderate anisocytosis and anisokaryosis and may be present in aggregates. A small amount of wispy to glassy, eosinophilic, extracellular matrix may be present, and nucleated cells may be found in close association with this matrix. Osteoclasts may be present in lesions with bone lysis or remodeling and appear as large, multinucleated cells with rounded or irregular cell borders, variable cytoplasmic projections, and basophilic cytoplasm with dark eosinophilic stippling (Figure 12.13). The nuclei are oval with reticular chromatin and a small, typically single nucleolus; the nuclei are typically fairly uniform in appearance within a cell. Osteoclasts may contain extremely variable numbers of nuclei; it is not uncommon to identify cells with more than ten nuclei and care must be taken not to confuse osteoclasts for neoplastic cells (Figures 12.13, 12.14a, b). 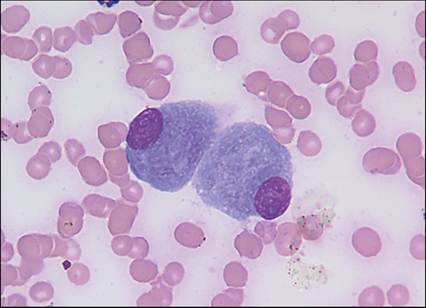
Figure 12.12 Reactive osteoblasts in a bone aspirate. The cells have a low N:C ratio, abundant basophilic cytoplasm, and a round, eccentric nucleus (Wright–Giemsa, 1,000? magnification). (Courtesy Anne Barger.)
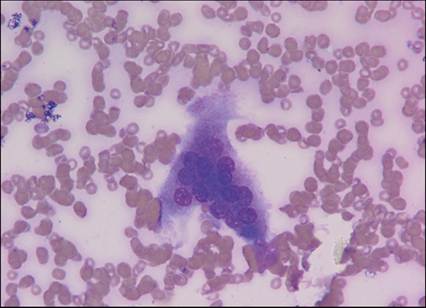
Figure 12.13 Osteoclast.
Large cell with variable borders and multiple uniform nuclei (Wright–Giemsa, 1,000? magnification). (Courtesy Anne Barger.)
On occasion, hematopoietic precursors will be observed in bone aspirates, particularly when lysis allows considerable penetration of the collecting needle into the medullary cavity.
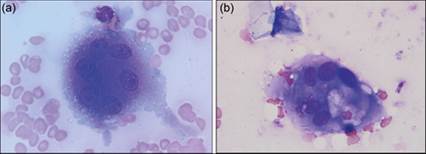
Figures 12.14a,b Osteoclast (a) and a neoplastic cell with multinucleation (b). Note the eosinophilic stippled cytoplasm and relative nuclear uniformity displayed by the osteoclast (Wright–Giemsa, both, 1,000? magnification). (12.14a courtesy Anne Barger.)
Inflammation
Inflammation of the bone is referred to as osteomyelitis. Inflammatory bone disease can be associated with lytic and/or proliferative lesions on radiographs, and lesions must be differentiated from similar radiographic findings that may be seen with a bone tumor. Aspirates of an inflamed bone may contain variable amounts of peripheral blood. In addition to disproportionately high numbers of leukocytes, the presence of degenerate neutrophils and phagocytic macrophages (as opposed to monocytes) can help differentiate inflammation from normal blood leukocytes. Careful review of the sample for infectious organisms should ensue. Identification of bacteria, particularly intracellular organisms, indicates the need for bacterial culture and susceptibility testing (Figure 12.15); culture of suppurative and pyogranulomatous bone lesions is also advisable when organisms cannot be identified. Several organisms have been associated with osteomyelitis, including Streptococcus spp., Nocardia spp., Mycobacterium spp., Bartonella spp., and Leishmania spp. (de Souza et al., 2005; Varanat et al., 2009; Lo et al., 2012; França et al., 2014; Hilligas et al., 2014). Lytic and proliferative lesions due to blastomycosis, histoplasmosis, coccidioidomycosis, cryptococcosis, and aspergillosis can be seen (Figures 12.16a–c; Walker et al., 2012; Block et al., 2017; Fielder et al., 2019; Shaver et al., 2022; Washington et al., 2022).
Pyogranulomatous inflammation is expected more commonly with fungal disease, although suppurative or chronic suppurative inflammation may also be observed (Figure 12.17). 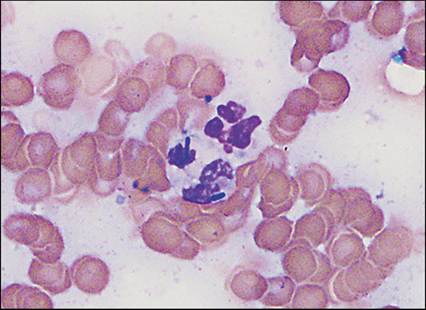
Figure 12.15 Septic osteomyelitis, with rod-shaped intracellular bacteria (Wright–Giemsa, 2,000? magnification).
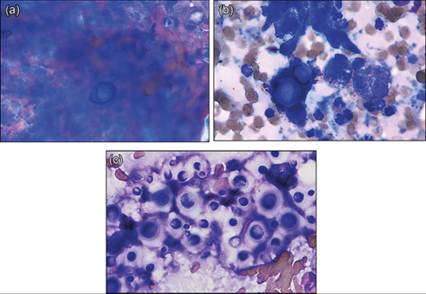
Figures 12.16a–c (a) Blastomyces dermatitidis (near bottom of image) with inflammatory cells. This fungal yeast is deeply basophilic staining, with a double-contoured cell wall, is typically 10–15 μm in diameter, and displays broad-based budding (not pictured). (Courtesy Anne Barger.) (b) Coccidioides spp. This fungus forms spherules that range in size from 10 to 200 μm in diameter. Endospores (2–4 μm) may be visible within larger forms or within the background on spherule rupture (not pictured). (Courtesy Anne Barger.) (c) Cryptococcus spp. The yeasts demonstrate the prominent mucoid capsule characteristic of this fungus. They typically display narrow-based budding and variable staining (Wright–Giemsa: a, 2,000? magnification; b and c, 1,000? magnification).
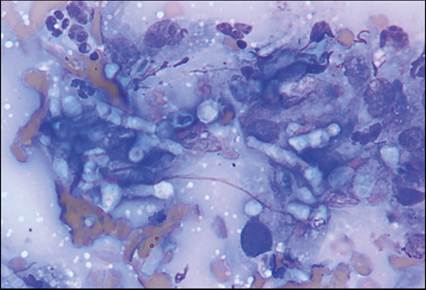
Figure 12.17 Fungal osteomyelitis in a dog. Lytic changes were noted on radiographs, and a bone neoplasm was suspected. Cytologic review of lesion aspirates revealed pyogranulomatous inflammation and fungal hyphae (Wright–Giemsa, 1,000? magnification). (Courtesy Anne Barger.)
Tumors of bone and cartilage
Osteosarcoma
Osteosarcoma is a malignant proliferation of osteoblasts. Osteosarcomas are often associated with concurrent bone proliferation. Many samples are a mixture of neoplastic and reactive osteoblasts, and differentiation of the two can prove challenging.
Additionally, reliable differentiation of osteosarcoma from other sarcomas based purely on cytologic appearance is typically not possible. The features of reactive osteoblasts have been described above. Neoplastic osteoblasts can display a range of atypia (Figures 12.18a, b). The cells may be rounded or spindloid in shape, with a small to large amount of basophilic cytoplasm. The cells may contain a few small (approximately 0.5–1 μm), rounded or angular, variably sized eosinophilic granules within the cytoplasm. The cells are expected to display variable degrees of anisocytosis, anisokaryosis, and anisonucleoliosis. The cells may be associated with a variable amount of wispy to glassy eosinophilic extracellular matrix, although this is not a criterion of malignancy and may also be seen in samples of reactive bone. The nuclei are often round or oval, and the chromatin pattern may range from fine to coarse to open, even within a single sample. Nucleoli are often prominent, multiple, and may vary considerably in size and shape. Erythrophagia may be observed within the cytoplasm of osteosarcoma cells but is not specific for this tumor type (Barger et al., 2012). Several subtypes of osteosarcoma exist and may influence cytologic sample features. A 2020 study that assessed 153 cases of canine osteosarcoma found osteoblastic osteosarcoma was the most common at 56.9%, followed by chondroblastic (13.7%), telangiectatic (11.8%), fibroblastic (7.8%), giant cell-rich (5.2%), and poorly differentiated neoplasms (4.6%) (Guim et al., 2020). Low case numbers among several subtypes precluded accurate determination of subtype influence on prognosis in this study.Once a diagnosis of sarcoma has been made on a bone aspirate, staining additional slides for alkaline phosphatase (ALP) activity can be helpful in differentiating between several types of sarcoma. This is evidenced by dark brown–black staining within the cytoplasm following incubation with nitroblue tetrazolium chloride/5-bromo-4-chloro-3-indolyl phosphate (NBT/BCIP) toluidine salt, which acts as a substrate for alkaline phosphatase in the cell (Barger et al., 2012).
Cells displaying significant criteria of malignancy, such as marked increases in the N:C ratio, multinucleation, or marked anisocytosis, must be confirmed positive to differentiate neoplastic cells from positively staining reactive osteoblasts that may also be present (Figure 12.18c). Osteoclasts are expected to be negative for alkaline phosphatase activity. Counterstaining of apparently negative slides with a Romanowsky stain is recommended to confirm that neoplastic cells are present. A study assessing the utility of ALP activity in differentiating between vimentin-positive tumors found that 33/33 osteosarcomas, 1/4 chondrosarcomas, and 1/1 multilobular tumor of bone were positive, while 3/4 chondrosarcomas, 2/2 fibrosarcomas of bone, 4/4 synovial cell sarcomas, and 2/2 plasma cell tumors were negative (Barger et al., 2005). Another study determined that slides previously stained with Wright–Giemsa could also be utilized for staining for ALP activity, allowing additional diagnostic testing on samples with limited cellularity (Ryseff & Bohn, 2012). This study found that 15/17 osteosarcomas were positive for ALP activity.A 2022 study assessing immunohistochemical staining of primary bone tumors found that sequential use of ALP, followed by the transcription factor runx2, provided 87% sensitivity and 85% specificity in distinguishing osteosarcoma from chondrosarcoma, fibrosarcoma, and histiocytic sarcoma; alone, ALP was highly sensitive (100%) but poorly specific (30%), and runx2 was moderately sensitive (87%) and specific (78%) (Barger et al., 2022).
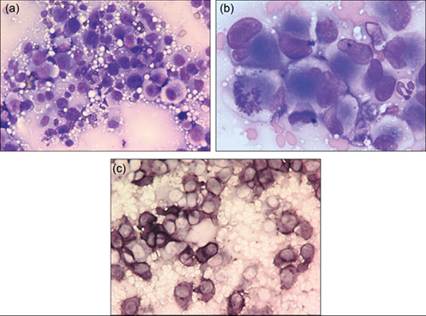
Figures 12.18a–c Osteosarcoma in a dog. (a, b) Pleomorphic rounded to spindloid cells (Wright–Giemsa: a, 500? magnification; b, 1,000? magnification). (c) Brown–black staining indicates ALP activity within the neoplastic cells. Criteria of malignancy should be identified within positive-staining cells to differentiate from reactive osteoblasts (NBT/BCIP, 500? magnification). (Courtesy Anne Barger.)
Chondrosarcoma
Chondrosarcomas (malignant proliferations of chondroblasts) are cytologically similar to osteosarcomas. Chondrosarcomas are often associated with a large amount of stippled to wispy, brightly eosinophilic, extracellular matrix (chondroid) that fills the background (Figures 12.19a, b). However, osteosarcomas and fibrosarcomas may also be associated with a significant amount of pink extracellular material. Chondrosarcomas tend to arise in the nasal cavity and in flat bones; a retrospective analysis of 31 cases of non-nasal chondrosarcomas in dogs found 13 cases occurred in appendicular long bones, 12 in ribs, 4 in the mandible, and 1 each in the maxilla and scapula (Waltman et al., 2007).
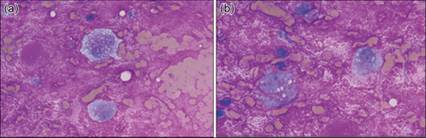
Figures 12.19a,b Chondrosarcoma in a dog. Pleomorphic mesenchymal cells within a distinctive background of thick, brightly eosinophilic, extracellular matrix (Wright–Giemsa: 1,000? magnification). (Courtesy Anne Barger.)