Campylobacter jejuni Infection
Campylobacter jejuni has been isolated on numerous occasions from clinically normal hamsters, as well as hamsters with enteritis. Hamsters acquired from pet stores have been found to be commonly infected with C.
jejuni. A few animals had watery diarrhea. Hamsters are relatively resistant to experimental disease. Manipulation may be required in order to produce clinical disease consistently in inoculated animals. Experimentally infected hamsters, which were preconditioned with magnesium sulfate as a purgative, were shown to develop edema, inflammation, and mild crypt hyperplasia of the ileal and cecal mucosa, with attachment of bacteria and disruption of the microvilli. Subclinically infected hamsters may shed the organism in the feces for up to several months. An outbreak of enterocecocolitis with mortality in a breeding colony of Syrian hamsters was attributed to concomitant infections with Escherichia coli and Campylobacter-like organisms. Adults were most frequently affected, and the cecum and colon were primarily involved. The organism can be a coinfecting pathogen during outbreaks of proliferative ileitis caused by Lawsonia intracellularis. Campylobacter-infected hamsters represent a zoonotic threat to both pet owners and laboratory animal personnel.Clostridium difficile Enterotoxemia
Dysbiosis due to disruption of the intestinal microflora of hamsters results in C. difficile enterotoxemia. The most common precipitating cause is treatment of hamsters with antibiotics, including lincomycin, clindamycin, ampicillin, vancomycin, erythromycin, cephalosporins, gentamicin, and penicillin. Typhlocolitis has been documented in hamsters, following topical treatment with antibiotic ointment containing polymyxin B sulfate, neomycin sulfate, and bacitracin zinc. Spontaneous enterotoxemia may also occur in hamsters in the absence of antibiotic treatment.
The exquisite susceptibility of hamsters to C. difficile enterotoxemia has made this species the primary animal model for study of this disease.Epizootiology and Pathogenesis
The predominant bacterial flora in the hamster intestine are Lactobacillus and Bacteroides. Following therapy with certain narrow-spectrum antibiotics, overgrowth with C. difficile occurs, resulting in acute typhlocolitis, diarrhea, and death. In general, profuse diarrhea, with high mortality, occurs within 2-10 days following the oral or parenteral administration of certain narrow-spectrum antibiotics. The oral administration of cecal contents from normal animals has provided protection to the majority of recipients. Change may be precipitated by the loss of Gram-negative aerobic bacteria or other Clostridia following antibiotic treatment, but dietary manipulation has also been shown to precipitate C. difficile enterotoxemia. Alteration of the “inhibitory barrier” of the microbiome may then allow colonization of C. difficile with elaboration of toxins A and B. Fatal typhlitis attributed to C. difficile has been observed in hamsters housed in the same room as antibiotic-treated hamsters. There is also some evidence that C. difficile
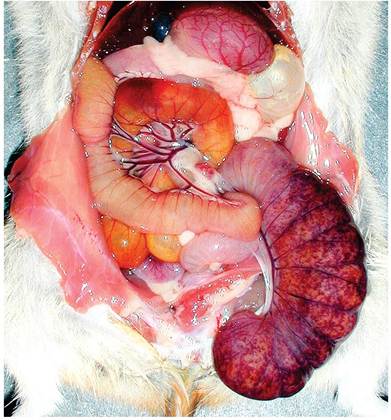
FIG. 3.8. Abdominal viscera of a hamster with Clostridium difficile enterotoxemia. Note the dilated bowel filled with fluid and the hyperemic and hemorrhagic cecum. Source: Keel and Songer. 2006. Reproduced with permission from SAGE Publications.
may occur as an endogenous infection, and the organism has been isolated from the intestinal tract of normal hamsters.
Pathology
The intestine may be distended with gas and tan to red fluid. The cecal wall may be hyperemic with ecchymotic hemorrhages (Fig. 3.8). There may be distension and hyperemia of the terminal ileum and proximal colon. Histopathologic lesions vary from mild to acute pseudomembranous necrohemorrhagic typhlitis (Fig. 3.9). Microscopic changes in the cecum include effacement of the mucosal epithelium, edema of the lamina propria, leukocytic infiltration, and mucosal hyperplasia. There may be some involvement of the terminal ileum and colon.
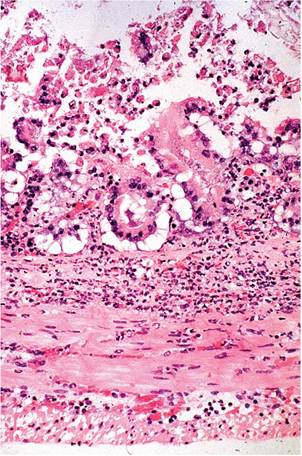
FIG. 3.9. Cecum from a hamster with spontaneous clostridial enteropathy not associated with prior antibiotic treatment. There is a necrotizing typhlitis with mucosal effacement and leukocytic infiltration.
Microscopic changes included hyperplasia of enterocytes lining cecal crypts, as well as focal mucosal erosions. Bacterial cultures and ultrastructural studies failed to identify a specific causative agent. The syndrome probably represents the recovery phase of clostridial enteropathy.