Carcinoids (neuroendocrine carcinoma)
Carcinoids are tumors of neuroendocrine cell origin that arise in multiple places throughout the body. They arise from enterochromaffin cells, which are present in the gastrointestinal (GI) tract, tracheobronchial tree, pancreatic ducts, biliary tree, and genitourinary tract (Giles et al., 1974).
In the GI tract, neuroendocrine cells are scattered throughout the mucosa and are normally responsible for the production of digestive hormones including secretin, somatostatin, and cholecystokinin, or they produce serotonin as part of the amine precursor uptake decarboxylation (APUD) group (Uzal et al., 2015). Neoplasms due to these cells are seen most commonly in the dog but have also been described in the cat; however, these are uncommon tumors in both species. GI carcinoids in dogs and cats have been described in the stomach, duodenum, jejunum, ileocecal junction, cecocolic junction, colon, and rectum (Giles et al., 1974; Patnaik et al., 1980a; Patnaik Lieberman, 1981; Sykes Cooper, 1982; Rossmeisl et al., 2002; Sako et al., 2003). Rectal carcinoids are occasionally seen as pedunculated lesions protruding from the rectum or anus, so they may be visualized during a physical examination or palpated during a rectal examination (Sykes Cooper, 1982). Metastatic lesions from GI carcinoids have been documented in the liver, lungs, heart, trachea, tonsils, pancreas, and mesenteric lymph nodes (Giles et al., 1974; Patnaik et al., 1980; Sako et al., 2003). Carcinoids in dogs and cats have also been described in the pancreas (Carakostas et al., 1979; Michishita et al., 2017) and in the gallbladder of dogs (O’Brien et al., 2021).Liver carcinoids make up approximately 13–14% of primary liver neoplasms in the dog. These lesions are often diffuse in dogs and cats, affecting multiple liver lobes, and >70% occur in dogs under 10 years of age (Patnaik et al., 1980; Patnaik, 1992).
Metastasis is reported in up to 93% of cases of hepatocellular carcinoid. When these lesions are found to have metastasized, the most common locations are the abdominal lymph nodes and peritoneum (Patnaik et al., 1980). Liver carcinoids have also been described in cats but with very low frequency (Patnaik, 1992; Meachem et al., 2016). Extrahepatic biliary carcinoids have also been described in dogs and cats (Patnaik, 1992; Morrell et al., 2002).Another location for carcinoid formation is the lungs, with rare canine reports available in the literature (Soo Choi et al., 2008) and a multi-institutional study showing these tumors make up 1.5% of primary lung tumors in dogs (McPhetridge et al., 2022). The most recent of these reports described cytologic findings that included large numbers of cell-free nuclei on a pale, basophilic background with a low number of intact, rounded cells (Figures 16.11a, b). The intact cells exhibit mild to rarely moderate anisocytosis, anisokaryosis, and variability in N:C ratio. The cells have a small to rarely moderate amount of lightly basophilic cytoplasm and a round, variably placed nucleus. The nuclei have finely stippled to reticular chromatin and inconspicuous nucleoli. In this report, the intact cells rarely had low numbers of small, basophilic cytoplasmic granules and a small amount of eosinophilic extracellular and intracellular material was noted (Soo Choi et al., 2008).
Neuroendocrine carcinomas have also been described in the perianal region in a cat (Joudrey et al., 2015), mammary gland of dogs (Nakahira et al., 2015; Nakagaki et al., 2021, 2022), kidney of a dog (Sozmen et al., 2020), and frontal sinus in a dog (Baek et al., 2019). Occasionally, neuroendocrine carcinomas are productive leading to clinical signs consistent with the overproduction of the associated hormone including a gastrinoma in a cat (Lane et al., 2016) and an ACTH producing sinusoidal neuroendocrine tumor in a dog (Baek et al., 2019).
Once histologic sections have been obtained, staining with specific silver stains to confirm the presence of argyrophil granules and/or argentaffin granules may be beneficial to obtain the diagnosis (Giles et al., 1974). Basic neuroendocrine markers, nonspecific enolase, chromogranin A, and synaptophysin may also be helpful (Patnaik, 1992; Sako et al., 2003; Soo Choi et al., 2008).
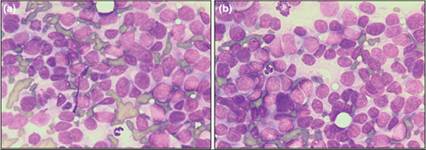
Figures 16.11a,b Carcinoid. Note the classic poorly preserved cell borders, mild anisocytosis and anisokaryosis, and the high nuclear to cytoplasmic ratio of the cells (Wright–Giemsa, 700? magnification).