Adrenal gland neoplasia
Hyperplastic and neoplastic lesions that may lead to enlargement of the adrenal glands and sampling for cytology may occur in the adrenal cortex or adrenal medulla. These lesions are often not palpated but are discovered during ultrasonography after patients are presented for clinical signs associated with hyperadrenocorticism or, less likely, clinical signs associated with hyperaldosteronism, hyperestrogenemia, or pheochromocytomas.
A retrospective study of dogs undergoing abdominal computed tomography showed 9.3% of dogs had incidental adrenal gland masses (Baum et al., 2016). Cytologic ability to differentiate adrenocortical neoplasia and pheochromocytoma has been found to have a high specificity and sensitivity (Bertazzolo et al., 2014), but differentiation between benign and malignant lesions is difficult. Fine-needle aspiration of the adrenal gland is a relatively safe procedure with a rare incidence of complications (Sumner et al., 2018; Pey et al., 2020). Hyperadrenocorticism may be suspected in dogs and cats that present for polyuria/polydipsia, polyphagia, a pot-bellied appearance, and poor hair coat, which are all secondary to increased glucocorticoid production. Clinical laboratory testing often shows no changes on the complete blood count, common serum biochemistry changes (hyperglycemia, increased alkaline phosphatase), and likely decreased urine specific gravity. Approximately 80–100% of cats with hyperadrenocorticism also have diabetes mellitus, which is often the initial diagnosis. Concurrent hyperadrenocorticism should be further investigated in cats for which large doses of insulin do not lead to control of clinical signs of diabetes mellitus (Waters Scott-Moncrieff, 2002). Since adrenal lesions in cats more commonly cause hyperaldosteronism, clinical signs may involve muscle weakness, plantigrade stance, problems jumping, and neck ventroflexion secondary to hypokalemia or signs of hypertension such as blindness due to retinal detachment or intraocular hemorrhage (Kooistra, 2020). At this point, advanced diagnostic testing, including dexamethasone suppression tests, adrenocorticotropic hormone (ACTH) stimulation test, and abdominal ultrasound, may be performed. There are two main causes for hyperadrenocorticism: a functional pituitary adenoma and a functional adrenal gland neoplasm of the adrenal cortex, located primarily in the zona fasciculata. A pituitary adenoma would lead to bilateral enlargement of the adrenal cortices secondary to continuous stimulation by ACTH. These types of lesions are often measured via ultrasonography but not sampled for cytology.Functional adrenal neoplasia only accounts for a small number of cases of hyperadrenocorticism (10–15%) in the dog (La Perle, 2011), with nonfunctional adrenal tumors and adrenal tumors that produce aldosterone also reported (Renschler & Dean, 2009). Functional adrenal tumors in cats typically produce aldosterone with those that produce cortisol or sex hormones (Guerios et al., 2015; Nadolski et al., 2016; Griffin, 2021) also possible. The median age for diagnosis of adrenal tumors is around 10.5–12 years in the dog (Labelle et al., 2004; Arenas et al., 2013). Adenomas are more frequent than carcinomas in dogs and often occur as single unilateral nodules (Miller, 2017). The literature on whether adenomas or carcinomas are more frequent in cats is conflicting (Daniel et al., 2016; Boland & Barrs, 2017) with adrenal neoplasia being extremely uncommon in cats (Griffin, 2021). Carcinomas are usually larger than adenomas and may be bilateral. The criteria that may be helpful to diagnose an adrenal carcinoma are tumor size >2 cm, increased cellular pleomorphism, hemorrhage, necrosis, capsular invasion, surrounding structure invasion, and vascular invasion (Labelle et al., 2004).
If an adrenal mass is noted, cytologic findings that would indicate adrenal cortical origin include a variable number of cell-free nuclei on a light purple background with a moderate amount of cell-free lipid.
Increased numbers of intact cells are noted compared with other endocrine neoplasms. The cells have a low to moderate N:C ratio and exhibit mild to rarely moderate anisocytosis and anisokaryosis. The cells have a moderate to abundant amount of lightly basophilic cytoplasm with variable numbers of punctate cytoplasmic vacuoles and a round, variably placed nucleus. The nuclei have coarse chromatin and a single small nucleolus. Adrenocortical carcinomas may show slightly more atypia, but well-differentiated lesions are also possible. The most common locations for metastasis of adrenocortical carcinoma are the liver and lungs (Labelle et al., 2004).Adrenal medullary lesions are often due to benign or malignant neoplastic proliferations of chromaffin cells, which are termed pheochromocytomas. Median age for occurrence of these tumors in dogs is 10.5 years, there is no breed or sex predilection, and approximately 50–60% are an incidental finding (Gilson et al., 1994; Barthez et al., 1997). Clinical signs suggestive of a functional pheochromocytoma are related to increased release of catecholamines (norepinephrine, epinephrine), leading to tachycardia, hypertension, and possibly neurologic abnormalities. The most common presenting complaints for dogs with a definitive diagnosis of pheochromocytoma include weakness/lethargy, polyuria/polydipsia, collapse, and vomiting; however, these findings may or may not be directly related to the tumor, as up to 50% of dogs have concurrent neoplasms (Barthez et al., 1997). Pheochromocytomas may also produce clinical signs secondary to a large, space-occupying mass in approximately 10% of cases including ascites, limb edema, abdominal pain, abdominal distension, and a palpable abdominal mass (Barthez et al., 1997). Measurement of plasma-free metanephrines, free metanephrine, and free normetanephrine may be appropriate, noninvasive diagnostic tests to help with the diagnosis of pheochromocytoma as well as the measurement of urine metanephrines (Gostelow et al., 2013; Salesov et al., 2015).
Adrenal medullary lesions are often large (>10 cm) single masses that may compress or completely replace the surrounding adrenal cortex (La Perle, 2011). Rare bilateral lesions are reported (Barthez et al., 1997). Criteria for diagnosis of malignant lesions are the same as those for carcinoma in other endocrine tumors (capsular and vascular invasion). The incidence of locally invasive lesions is reported as 39–50%, and metastasis is reported in 13–28% of cases (Gilson et al., 1994; Barthez et al., 1997). Previously reported metastatic sites in the dog include the liver, lungs, regional and distant lymph nodes, spleen, kidney, prostate, bone, pancreas, peritoneum, spinal canal, brain, caudal vena cava, heart, and jejunum (Gilson et al., 1994; Barthez et al., 1997; Boes et al., 2009b; Machida Machida, 2020; Gregor et al., 2022). Cytologic findings include a highly cellular sample composed of sheets of rounded cells with poorly distinct cell borders and large numbers of cell-free nuclei (Figures 16.10a–d). The cells have a rarely moderate to high N:C ratio and exhibit mild to rarely moderate anisocytosis and anisokaryosis. The cells have a small to rarely moderate amount of lightly basophilic cytoplasm and a round, central nucleus. The nuclei have finely stippled to rarely reticular chromatin and occasionally a single small nucleolus. Immunocytochemical staining that may be beneficial to confirm the chromaffin origin of cells from an adrenal mass include chromogranin A and synaptophysin, although not all tumors may stain with both markers (Barthez et al., 1997).
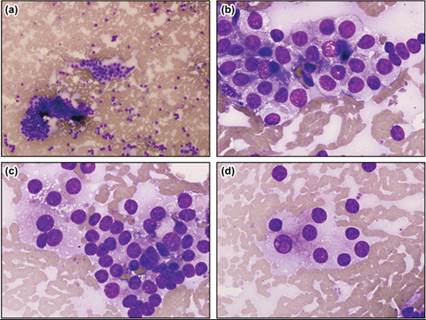
Figures 16.10a–d Adrenal medullary mass. Cat. Aspirates of a mass in the left adrenal gland that measured 2.6 cm ? 2.5 cm on ultrasound. Increased levels of normetanephrine and metanephrine were documented (Wright–Giemsa: a, 100? magnification; b–d, 1,000? magnification).
Other than tumors of the predominant cellular components of the adrenal gland, few reports of other primary lesions and metastatic lesions within the adrenal gland have been published. Additional primary adrenal gland neoplasms that have been previously described include myelolipomas (Tursi et al., 2005), neuroblastomas (Marcotte et al., 2004; Mestrinho et al., 2019), lymphoma (Romine et al., 2016) malignant peripheral nerve sheath tumor (Ichikawa et al., 2018), and ganglioneuromas (Miller, 2017). The rate of metastasis to the adrenal gland in the dog has been documented as 21% and in the cat as 14.8% (Labelle De Cock, 2005). In terms of metastatic lesions accounting for adrenal tumors, they make up 26.7% of adrenal tumors in the dog and 60% in the cat (Labelle De Cock, 2005). The metastatic lesions are bilateral in approximately 50% of cases in dogs and cats (Labelle De Cock, 2005).
More on the topic Adrenal gland neoplasia:
- Adrenal gland neoplasia
- References
- Introduction
- Barger A.M., MacNeill A.L. (Eds.). Small Animal Cytologic Diagnosis: Canine and Feline Disease. CRC Press,2024. — 536 p., 2024
- Chapter summary
- Necropsy: The Postmortem Examination