Cases
CASE 1
Signalment/history
A 10-year-old, spayed female mixed-breed dog presented with a palpable ventral neck mass.
Cytology
The mass was aspirated. The sample was markedly hemodiluted.
Clusters of neoplastic epithelial cells were observed. These cells were round with a moderate amount of basophilic cytoplasm and indistinct cell borders (Figure 16.12). The nuclei were round with coarsely stippled chromatin pattern and small but prominent nucleoli. A few cells contained pigmented granular material within the cytoplasm (Figure 16.13). Cytologically, this sample was consistent with thyroid neoplasia. Although the cells do not exhibit many criteria of malignancy, thyroid carcinoma is likely. 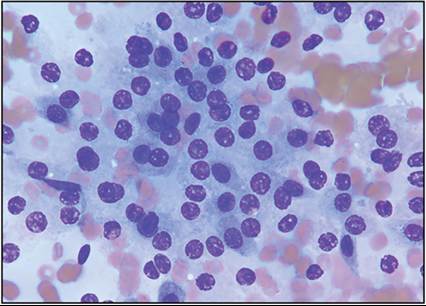
Figure 16.12 Aspirate from the ventral neck mass. A cluster of neoplastic epithelial cells is present with indistinct cytoplasmic borders. The overall cell population is fairly uniform with only mild anisokaryosis (Wright–Giemsa, 700? magnification).
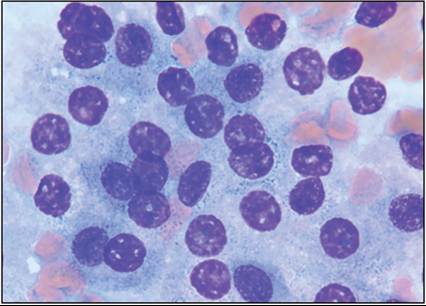
Figure 16.13 Occasionally, cells contained a few basophilic granular structures within the cytoplasm (Wright–Giemsa, 1,500? magnification).
Management
The mass was surgically excised and diagnosed as a thyroid carcinoma.
CASE 2
Signalment/history
A 6-year-old, male castrated English Bulldog presented for a suspected gallbladder mucocele. The dog had a three-week history of intermittent anorexia, vomiting, and melena. The referring veterinarian identified a gallbladder mass on abdominal ultrasound.
Cytology
The mass was aspirated. The smears were very low in nucleated cellularity with mild to moderate blood contamination. One smear was moderately cellular and contained several cohesive sheets of cells with poorly distinct cell borders and mild to rarely moderate anisokaryosis. The nuclei were round with lacy chromatin and inconspicuous nucleoli.
The cells have a moderate amount of basophilic cytoplasm (Figure 16.14). 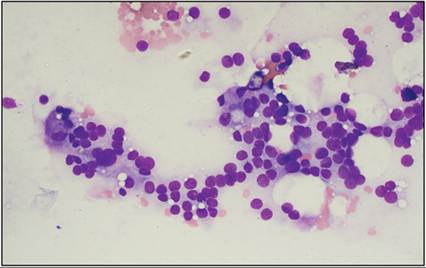
Figure 16.14 Aspirate from an intraluminal gallbladder mass. A loosely cohesive sheet of neoplastic cells is present with indistinct cell borders and mild anisokaryosis (Wright–Giemsa, 500? magnification, courtesy of Dr. Michael Rosser and Dr. Taylor Hanson).
Management
The patient underwent surgery, and the entire gallbladder was removed and submitted for histopathology. Histopathologic evaluation showed an unencapsulated and invasive mass expanding and effacing the gallbladder submucosa. The mass was composed of cells in nests, packets, and sheets suggestive of an epithelial tumor (Figure 16.15). Additional immunostaining was performed with synaptophysin, which was positive (Figure 16.16), and cytokeratin, which was negative. These results indicated a neuroendocrine carcinoma.
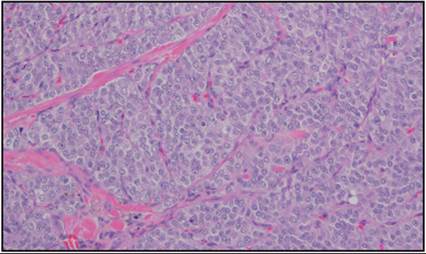
Figure 16.15 Histopathology of a gallbladder mass. The cells are arranged in nests, packets, and sheets and show mild anisocytosis and anisokaryosis (hematoxylin and eosin, 100? magnification, courtesy of Dr. Patrick Roady).
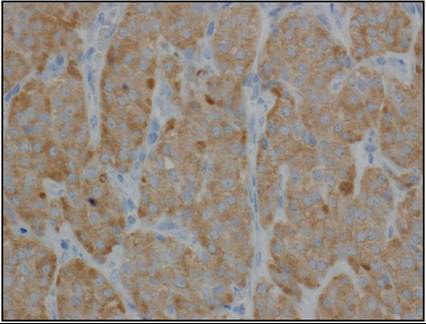
Figure 16.16 Histopathology of a gallbladder mass. The cells label positive for synaptophysin which is indicative of neuroendocrine origin (HRP polymer mouse monoclonal antibody with DAB chromogen and hematoxylin counter stain, 400? magnification, courtesy of Dr. Patrick Roady).