Combined hepatocellular-cholangiocarcinoma
Combined hepatocellular-cholangiocarcinoma is very infrequently encountered. It makes up 2–5% of primary canine liver tumors. Some of the neoplastic cells have a hepatocellular morphology while others have a distinctly biliary morphology (Terai et al., 2022).
Grossly, the lesions are typically large and have cystic regions. The reported prognosis after surgical excision is good.Biliary epithelium origin tumors
Benign bile duct tumors have variably been called biliary adenoma, biliary cystadenoma, cholangiocellular adenoma, and cholangioma histologically, while the malignant form has been called biliary carcinoma, cholangiocarcinoma, and cystadenocarcinoma depending on their architectural morphology and an uncertain understanding of the cell of origin. These distinctions cannot usually be made on cytologic evaluation.
Cytologically, neoplastic biliary epithelium commonly looks benign, irrespective of its actual clinical course. Cohesive structures that represent all morphologic features of the biliary tree can be observed, including clusters, tubules, sheets, and acinar arrangements (Figures 9.37a–c, 9.38a, b). The individual cells will frequently have less cytoplasm than a hepatocyte, making the cells appear more densely packed together. Depending on secretory function, there may be minimal to prominent vacuolation within the basophilic cytoplasm. Neoplasms that are cystic or highly secretory can be associated with either bile fluid or mucinous material, and aspiration of significant amounts of fluid can be achieved.
Benign biliary neoplasia is rarely observed in dogs, but is the most common primary hepatic tumor in the cat (Trigo et al., 1982). Large fluid-filled cystadenomas have measured up to 8 cm. Many incidental cystadenomas have been reported; clinical signs, when present, are often caused by the mass acting as a space-occupying lesion (Nyland et al., 1999).
Malignant biliary neoplasia is more commonly observed in the dog and less commonly observed in the cat. This tumor tends to behave aggressively with 60–80% metastatic rates and spread to the local lymph node, lung, abdominal organs, and bone (Balkman, 2009). 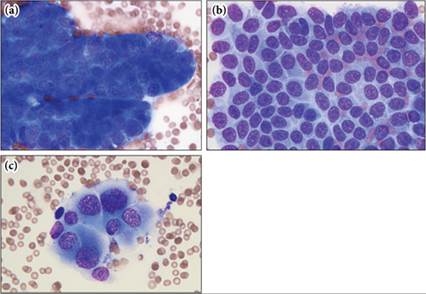
Figures 9.37a–c (a) Large papillary structures are evident in this aspirate from a domestic shorthair cat with ultrasonographically confirmed hepatic nodules. (b) Sheets of cells help confirm that the population is predominantly cuboidal with minimal to moderate amounts of cytoplasm. (c) Cells with moderate anisocytosis and anisokaryosis are abundant. The cell morphology is most consistent with biliary origin. Although cats most commonly have benign biliary neoplasms, the criteria of malignancy noted here lead to the concern that this is a carcinoma. Biopsy and histopathology should be performed to make this distinction (Wright–Giemsa, 1,000? magnification).
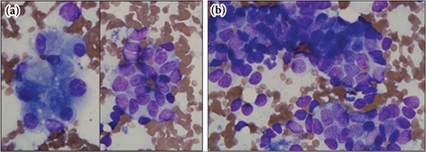
Figures 9.38a,b (a) Contrast the hepatocytes on the left with the cuboidal epithelial cells on the right in this feline sample. The cuboidal cells are most consistent with biliary epithelium. (b) Many cells are ruptured but where intact they were found in large clusters. The pleomorphism noted suggests a biliary neoplasm, which is most likely a benign neoplastic process (Wright–Giemsa, 1,000? magnification).