Cystic hyperplasia of the biliary system
Increased numbers of cytologically normal biliary epithelial cells suggest cholestasis and biliary hyperplasia (Stockhaus et al., 2004). Additionally, cirrhosis results in a relative decrease in hepatocytes which produces the appearance of increased numbers of biliary epithelium and can have concurrent biliary hyperplasia (Stockhaus et al., 2004).
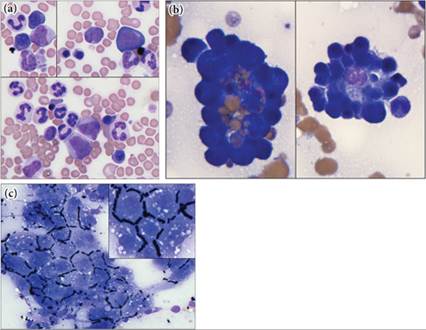
The hyperplastic progress can advance to a more easily diagnosed cystic hyperplasia of the biliary system. This is seen as larger accumulations of biliary epithelium, bile pigment, and aggregates of blue to blue–gray mucoid material (so-called white bile [Figures 9.22a–g]; Stalker & Hayes, 2007). Experimental studies demonstrate an association between exposure to bile salts and hyperplastic and secretory activity of biliary epithelium, implicating cholestasis as a potential initiating cause of cystic hyperplasia (Klinkspoor et al., 1995; Lamote Willems, 1997). Additionally, genetic causes may play a factor; Cocker Spaniels, Shetland Sheepdogs, and Miniature Schnauzers are more predisposed to biliary mucoceles (Pike et al., 2004).
Amyloid
Under certain conditions, proteins that are normally expressed in the body (e.g. serum amyloid A, immunoglobulin light chain, prion protein, and atrial natriuretic peptide, among others) can form characteristic beta pleated sheets, bind serum amyloid P, and be deposited on basement membranes. Although the substrate proteins are vastly different, at a microscopic level this material is visually indistinguishable and is collectively called amyloid. With Romanowsky staining, hepatic amyloid appears as pink fibrillar extracellular material closely associated with hepatocyte clusters. The beta pleated sheet arrangement of amyloid produces characteristic birefringence after staining with Congo red and visualization with polarized light (Beatty et al., 2002).
Amyloid deposition is not limited solely to the liver, but commonly involves the kidney, central nervous system, spleen, lung, pancreas, and several other organs (Segev et al., 2012).Amyloidosis has been classified as immunoglobulin-related (primary), reactive (secondary), and familial. Siamese and related breeds, Abyssinian cats, and Chinese Shar-Pei dogs have confirmed familial forms of amyloidosis (AA type amyloidosis), each with a specific amino acid substitution (Niewold et al., 1999; Segev et al., 2012). Half of dogs with amyloidosis had a history of infectious disease, and another quarter of the patients had a noninfectious, inflammatory disease, demonstrating the multifactorial nature of this disease (Segev et al., 2012).
Insufficient data are available to characterize the accuracy of cytology at identifying hepatic amyloidosis, as the cytologically described cases are presented as single case studies in the literature and not as a case series (Roth, 2001; Meyer, 2010). Suffice it to say that amyloid can be observed cytologically, but a lack of amyloid does not rule out amyloidosis.
Extramedullary hematopoiesis
Embryologic hepatoblast cytokine production induces the niche necessary to make the liver the first site of hematopoietic production (Sugiyama et al., 2011). Under conditions of increased hematopoietic need in the adult, this capacity is revived and manifests as the development of both erythroid, myeloid, and/or megakaryocytic cell proliferation associated with resident Kupffer cells (Figures 9.23a–c; Otsuka et al., 2011). Although the cytologic diagnosis of extramedullary hematopoiesis (EMH) can be made based on the presence of any one hematopoietic cell line with complete maturation outside the bone marrow, EMH of multiple cell lines is commonly seen. EMH, like lipid and glycogen accumulation, is a fairly nonspecific finding. It should be considered a secondary change and an aid to help define the nature of the primary problem. Care should be taken to ensure that the sample is truly representative of the liver, as incidental aspiration of the spleen during hepatic FNA is common (colloquially termed a ‘spliver’ sample by the author) and the spleen is a more common site of EMH.
Hepatic EMH produces a multifocal to diffuse ultrasonographic lesion, and therefore a higher cytologic accuracy for this entity could be predicted; however, data hint at poor diagnostic performance in small study populations (Warren-Smith et al., 2012; Bahr et al., 2013). Myelolipoma is an uncommon benign tumor, which presents as a nodular lesion with bone marrow elements and adipocytes cytologically. Myelolipoma can be challenging to distinguish from EMH by aspiration alone. 
Figures 9.22a–g Domestic shorthair cat with benign biliary hyperplasia confirmed by clinical progression and histology. (a) Rafts of biliary epithelium, which are columnar to cuboidal with basophilic to pink granular cytoplasm and mild dysplastic changes, including mild anisocytosis and variable N:C ratio, are present (Wright–Giemsa, 1,000? magnification). (b) Occasionally, these cells are found in balls and acinar-like structures around a center of blue secretory material (Wright–Giemsa, 1,000? magnification). (c) Lightly basophilic to gray extracellular material, white bile, is often found within some of these cell clusters and free in the background (Wright–Giemsa, 500? magnification). (d) White bile can cause the red blood cells to line up in linear arrangements, called windrowing. Dark blue–black material is found within cells and extracellularly. A few macrophages also display erythrophagocytosis (lower left corner) (main image, Wright–Giemsa, 1,000? magnification; inset, Wright–Giemsa, 200? magnification). (e) Columnar biliary epithelium, pigment-laden macrophages, and a single bright orange rhomboidal hematoidin crystal are present. Large hematoidin crystals are three-dimensional structures and therefore can lie in a different plane of focus from the surrounding cells (inset). Hematoidin usually suggests chronic hemorrhage but can be part of normal bile fluid (Wright–Giemsa, 1,000? magnification).
(f, g) Interestingly, most of the material in this sample is Prussian blue negative, demonstrating that the blue–black material seen here is predominantly bile with minimal hemosiderin (f, Wright–Giemsa, 1,000? magnification; g, Prussian blue, 1,000? magnification; inset is from the control sample, iron forms a blue pigment with this reaction).
Figures 9.23a–c Liver aspirate from a 4-year-old mixed breed dog with ultrasound confirmed liver nodules. (a) Extramedullary hematopoiesis is noted by the presence of both myeloid and erythroid lineages in the sample. The upper left inset contains (from upper left to lower right) a segmented neutrophil, two basophilic rubricytes, a promyelocyte, a band neutrophil, and a clump of platelets. The upper right inset contains (from left to right) a metarubricyte, a polychromatophilic rubricyte, a myeloblast, a rubriblast, a band neutrophil, and two segmented neutrophils. The lower panel contains (from upper left to lower right) seven segmented neutrophils surrounding a polychromatophilic rubricyte, a small lymphocyte, a myelocyte, two promyelocytes, a basophilic rubricyte, a large segmented neutrophil, and a polychromatophilic rubricyte. Note the large platelet along the right side of the image, which is roughly the size of the surrounding RBCs (Wright–Giemsa, 1,000? magnification). (b) Two erythroid islands, composed of maturing erythrocytes surrounding a supporting histiocytic/dendritic cell (likely a Kupffer cell). The histiocytic cell, also sometimes called a nurse cell, can be erythrophagic (Wright–Giemsa, 1,000? magnification). (c) The hepatocyte clusters in this patient had prominent bile casts that beautifully highlight the polygonal nature of the hepatocytes (Wright–Giemsa, 500? magnification; inset, 1,000? magnification).
Necrosis
When a pathologic process pushes the microenvironment sufficiently away from homeostasis, necrosis will ensue.
Necrotic but still intact cells will have a lack of cytoplasmic detail and condensed or karyorrhectic nuclei (Figure 9.24). This is apparent on cytology as basophilic amorphous to granular acellular debris (Figure 9.25). Necrotic material can be seen with infectious etiologies and within the poorly vascularized center of mass lesions. Often, re-aspiration of the margin of a lesion that previously produced necrotic debris will help identify the pathologic process leading to the necrosis. 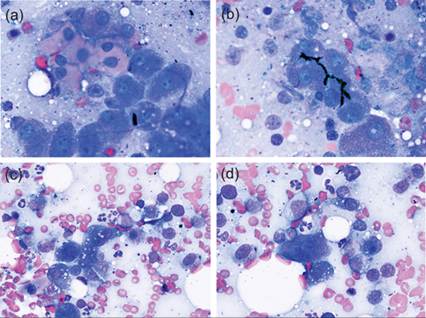
Figures 9.24a–d Liver aspirates from a 7-year-old neutered male Golden Retriever dog with an acute history of inappetence, lethargy, and depression. (a) Individualized cells with smooth pink cytoplasm and a slightly condensed nucleus suggest single cell necrosis. Note the continuum between these cells and the hepatocytes, helping to confirm the origin of the cell population. (b) Bile casts are present and indicate cholestasis. (c&d) A mixed population of neutrophils, macrophages, and lymphocytes surround hepatocytes and a fusiform fibroblast (d) is present (Wright–Giemsa, 1,000? magnification).
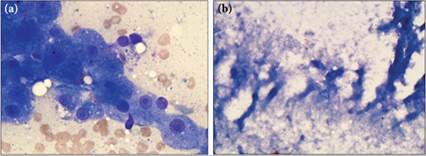
Figures 9.25a,b (a) A few clusters of intact and fairly normal hepatocytes are present from this dog (Wright–Giemsa, 1,000? magnification). (b) However, several slides contain abundant blue–gray acellular granular necrotic material. Note the ovoid structures, which may once have been nuclei. Mononuclear inflammation was present in the sample (not shown) and may have been responding to the necrosis or the process that instigated the necrosis (Wright–Giemsa, 500? magnification).
Fibroplasia
Hepatic fibrosis results from chronic inflammation within the liver (Eulenberg et al., 2018). Histologically, there is an expansion of the number of spindled mesenchymal cells, mast cells, and collagenous extracellular matrix.
Several clinically different histologic patterns of fibrosis can occur (portal-portal, portal-centrilobular, centrilobular-centrilobular, dissecting fibrosis). The degree of fibrosis is clinically relevant. Importantly, fibrosis is a component of chronic hepatopathy and is a sequelae of extrahepatic bile duct obstruction, cholangitis, increased central venous pressure due to right-sided heart failure, or other causes (Eulenberg et al., 2018). Congenital abnormalities, including polycystic kidney disease in cats, can induce hepatic fibrosis (Bosje et al., 1998). Hepatic fibrosis is an important event in the progression to cirrhosis and is associated with prognosis (Sevelius et al., 1995).Cytologic evidence for hepatic fibroplasia is the presence of increased numbers of spindled cells associated with pink fibrillar extracellular material that often trails out of the hepatocyte cluster (Figure 9.26). Cytologic preparations from hepatic fibrosis are expected to have increased numbers of individualized and minimally pleomorphic mast cells. One study found that cytologic smears from cases with hepatic fibrosis had >10% spindled cells and >4% mast cells across 10 high-powered fields (Masserdotti et al., 2016). Because of the limitations of fine needle aspiration, the pattern and degree of fibrosis cannot be determined from cytologic evaluation, but there has been suggestion that evaluation of serum biomarkers, including a proprietary algorithm of markers commonly included in serum biochemistry profiles, can provide information on the stage of fibrosis (Eulenberg et al., 2018; Menard et al., 2019).
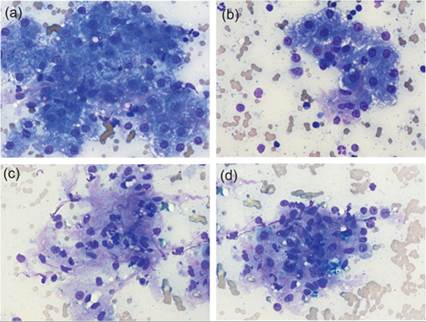
Figures 9.26a–d Liver aspirate from a 15-year-old domestic medium-haired cat. (a) Clusters of minimally pleomorphic hepatocytes with cytoplasmic rarefaction are present. Strands of pink fibrillar material are present within the clusters. (b) Cells with longer and slightly more condensed nuclei are more apparent within this cluster. (c) Larger aggregates of the extracellular material and spindled mesenchymal cells are present and few neutrophils are found within this aggregate. (d) Additionally, areas with macrophages are found within the mesenchymal component of this sample. Flow cytometry and PARR analysis (PCR for antigen receptor rearrangement) suggested a clonal CD21+ lymphocytosis from the concurrently submitted mesenteric lymph node aspirate. The neoplastic population was not apparent by cytology and the evidence of fibroplasia was considered an incidental finding (Wright–Giemsa, 500? magnification).
Inflammatory processes
Given the bloody background of many hepatic biopsy samples, merely observing leukocytes in liver cytology is insufficient evidence of inflammation. Cytologic diagnosis of inflammation in the liver should be based on the presence of increased numbers of leukocytes relative to peripheral blood or consistent observation of inflammatory cells within or associated with clusters of hepatocytes. Different pathologic processes are more commonly associated with inflammation in specific regions of the liver, but this information is not available from cytology. Notwithstanding, significant information can be gained cytologically, which can aid in the determination of subsequent diagnostic steps to fully understand the cause of inflammation.